
The human immunodeficiency virus (HIV) is a type of virus called a retrovirus, which can infect humans when it comes in contact with tissues that line the vagina, anal area, mouth, eyes, or through a break/cut/wound in the skin. Human Immunodeficiency Virus or HIV infection if left untreated causes AIDS (acquired immunodeficiency syndrome).
HIV infection is generally a slowly progressive disease in which the virus is present throughout the body at all stages of the disease.
Stages
Three stages of HIV infection have been described:
- The initial stage of infection (primary infection), which occurs within weeks of acquiring the virus, often is characterized by the flu- or mono-like illness that generally resolves within weeks.
- The stage of chronic asymptomatic infection (meaning a long duration of infection without symptoms) lasts an average of eight to 10 years without treatment.
- The stage of symptomatic infection, in which the body’s immune system has been suppressed and complications have developed, is called the acquired immunodeficiency syndrome (AIDS – In AIDS, the immune system collapses, and the body falls prey to secondary, opportunistic infections and cancers that typically kill the person).
The symptoms are caused by the complications of AIDS, which include one or more unusual infections or cancers, severe loss of weight, and intellectual deterioration (called dementia).
When HIV grows it mutates (acquires the ability to change) its own structure. These mutations enable the virus to become resistant to previously effective drug (allopathic only) therapy.
Diagnosis
The test that for decades had been most commonly used for diagnosing infection with HIV was referred to as an ELISA. If the ELISA found HIV antibodies, the results needed to be confirmed, typically by a test called a Western blot. Antibodies to HIV typically develop within several weeks of infection. During this interval, patients have virus in their body but will test negative by the standard antibody test, the so-called “window period.” In this setting, the diagnosis can be made with tests for HIV RNA or p24 antigen. If the confirmatory antibody test is negative, then there remains the possibility that the original test detected viral p24 antigen and not antibodies, and therefore infection still is likely.
How does HIV spread?
HIV is present to variable degrees in the blood and genital secretions of virtually all untreated  individuals infected with HIV, regardless of whether or not they have symptoms. The spread of HIV can occur when these secretions come in contact with tissues especially mucus membrane (vagina, anal area, mouth, eyes), or with a break in the skin, such as from a cut or puncture by a needle. The most common ways in which HIV is spreading throughout the world include sexual contact, sharing needles, and by mother-to-child transmission during pregnancy, labor, very rarely breastfeeding.
individuals infected with HIV, regardless of whether or not they have symptoms. The spread of HIV can occur when these secretions come in contact with tissues especially mucus membrane (vagina, anal area, mouth, eyes), or with a break in the skin, such as from a cut or puncture by a needle. The most common ways in which HIV is spreading throughout the world include sexual contact, sharing needles, and by mother-to-child transmission during pregnancy, labor, very rarely breastfeeding.
Sexual transmission of HIV has been described from men to men, men to women, women to men, and women to women through vaginal, anal, and oral sex; through touching of tears and/or nasal discharges of infected person, through shearing/using things etc.
The spread of HIV by exposure to infected blood usually results from sharing needles, as in those used for illicit drugs. HIV also can be spread by sharing needles for anabolic steroids to increase muscle, blood transfusions, tattooing, and body piercing etc.
Recent data has demonstrated that if a person’s plasma viral load is consistently undetectable for at least 6 months of therapy, there is no longer any risk of sexually transmitting HIV to their spouses, leading to the phrase that undetectable equals untransmutable (although in most studies undetectable is defined as viral loads of < 200-400 copies/mL).
Signs and symptoms of Human Immunodeficiency Virus
The time from HIV infection to the development of AIDS varies. Rarely, some individuals develop complications of HIV that define AIDS within one year, while others remain completely asymptomatic after as many as 20 years from the time of infection. However, in the absence of antiretroviral therapy, the time for progression from initial infection to AIDS is approximately eight to 10 years. The reason why people experience clinical progression of HIV at different rates remains an area of active research.
Within weeks of infection, many people will develop the varied symptoms of primary or acute infection, which typically has been described as a mononucleosis– or influenza-like illness but can range from minimal fever, aches, and pains to very severe symptoms.
The most common symptoms of primary Human Immunodeficiency Virus infection are:
- fever,
- aching muscles and joints,
- sore throat, and
- swollen glands (lymph nodes) in the neck.
It is not known, however, why only some HIV-positive people develop these symptoms. It also is also not completely known whether or not having the symptoms is related in any way to the future course of HIV disease. Regardless, infected people will become asymptomatic after this phase of primary infection. During the first weeks of infection when a patient may have symptoms of primary HIV infection, antibody testing may still be negative (the so-called window period). If there is suspicion of early infection based upon the types of symptoms present and a potential recent exposure, consideration should be given to having a test performed that specifically looks for the virus circulating in the blood, such as a viral load test or the use of an assay that identifies HIV p24 antigen, for example, the new fourth-generation antibody/antigen combination test.
PrimaryHIV
Identifying and diagnosing individuals with primary infection is important to assure early access into care and to counsel them regarding the risk of transmitting to others. The latter is particularly important since patients with primary HIV infection have very high levels of virus throughout their body and are likely to be highly infectious.
There is no definitive data showing that initiation of allopathic antiretroviral therapy during this early stage of infection results in clinical benefits. However, there are many proven, treated cases with Homeopathic medicines. 
Nevertheless, it is generally thought that the benefits of reducing the size of the HIV in the body, preserving select immune responses, and reducing transmissibility favors early treatment. Once the patient enters the asymptomatic phase, infected individuals will know whether or not they are infected if a test for HIV antibodies is done.
Stage 2
Shortly after primary infection, most HIV-positive individuals enter a period of many years where they have no symptoms at all. During this time, CD4 cells may gradually decline, and with this decline in the immune system, patients may develop the mild HIV symptoms and signs such as vaginal or oral candidiasis thrush, fungal infections, a white brush-like border on the sides of tongue called hairy leukoplakia, chronic rashes, diarrhea, fatigue, and weight loss.
Any of these symptoms should prompt HIV testing if it is not being done for other reasons. With a further decline in function of the immune system, patients are at increasing risk of developing more severe complications of HIV, including more serious infections (opportunistic infections), malignancies, severe weight loss, and decline in mental function.
From a practical perspective, most physicians think about patients with HIV diseases as having no symptoms, mild symptoms, or being severely symptomatic. In addition, many would characterize a patient’s level of immunosuppression by the degree and type of symptoms they have as well as the CD4 cell count.
Specific diseases
Researchers defined the presence of a long list of specific diseases or the presence of less than 200 CD4 cells per mm3 as meeting a somewhat arbitrary definition of AIDS. It is important to note that with effective antiretroviral therapy especially Homeopathic, many of the signs and symptoms of HIV as well as severity of immunosuppression can be completely reversed, restoring even the most symptomatic patients to a state of excellent health.
Laboratory tests for Human Immunodeficiency Virus
One of the tests, which counts the number of CD4 cells, assesses the status of the immune system. The other test, which determines the so-called viral load, directly measures the amount of virus in the blood.
The CD4 count in the blood is normally above 400 cells per mm3 of blood. A declining number of CD4 cells means that HIV disease is advancing. Thus, a low CD4 cell count signals that the person is at risk for one of the many opportunistic infections that occur in individuals who are immunosuppressed.
Drug-resistance testing also has become a key tool in the management of HIV-infected individuals. Resistance testing is now routinely used in individuals experiencing poor responses to HIV therapy or treatment failure. In general, a poor response to initial treatment would include individuals who fail to experience a decline in viral load of approximately hundredfold in the first weeks, have a viral load of greater than 500 copies per mL by week 12, or have levels greater than 50 copies per mL by week 24.
Treatment failure would generally be defined as an increase in viral load after an initial decline in a person who is believed to be consistently taking his or her medications.
Allopathic treatment for Human immunodeficiency virus or HIV
There is no evidence that people infected with HIV can be cured by the currently available allopathic therapies. Allopathic therapy must balance the risk versus the benefits of treatment. The risks of therapy include the short- and long-term side effects of the drugs, described in subsequent sections, as well as the possibility that the virus will become resistant to the allopathic therapy.
If the virus remains detectable on any given regimen, resistance eventually will develop. Indeed, with certain drugs, resistance may develop in a matter of weeks, such as with the nucleoside reverse transcriptase inhibitors (NRTIs) lamivudine (Epivir, 3TC) and emtricitabine (Emtriva, FTC), the drugs in the class of nonnucleoside analogue reverse transcriptase inhibitors (NNRTI) such as nevirapine (Viramune, NVP), delavirdine (Rescriptor, DLV), efavirenz (Sustiva, EFV), rilpivirine (Edurant, RPV), and doravirine (Pifeltro, DOR) as well as the integrase strand transfer inhibitors (InSTIs) such as raltegravir (Isentress, RAL) and elvitegravir (Vitekta, EVG).
If these drugs are used as part of a combination of agents that do not suppress the viral load to undetectable levels, resistance will develop, and the treatment will lose its effectiveness. In contrast, HIV becomes resistant to other drugs, such as the boosted protease inhibitors (PIs), over months. Resistance also seems to be relatively uncommon with the newer InSTIs, such as dolutegravir (tivicay, DTG) and bictegravir (BIC), which is only available as a combination pill (Biktarvy) with tenofovir alafenamide (TAF) and emtricitabine (FTC).
What factors should be considered before starting antiviral therapy?
Until very recently, one of the biggest questions related to the management of HIV disease was the optimal time to start allopathic antiviral treatment. For some time, there had been very strong data demonstrating that therapy is appropriate for those with CD4 cells numbering less than 350 cells/mm3 in the blood. There have also long been strong recommendations to treat patients with select conditions regardless of their CD4 cell count, such as during pregnancy in order to prevent transmission of HIV to the baby or those who have HIV-associated renal disease or chronic hepatitis B infection where the antiviral treatment for HIV also treats the hepatitis virus.
There are now several very large studies that have shifted all guidelines around the world to recommending allopathic treatment of all HIV-infected individuals at the time of diagnosis no matter what the CD4 cell count. Regardless, prior to initiating antiviral therapy, everything possible should be done to ensure that the patient is committed to the treatment, able to adhere to the regimen, and will follow up with his or her health care professional to assess whether medications are tolerated and working.
Initial allopathic therapy
Antiviral treatment options have primarily included combinations of two NRTIs, often referred to as “nucs,” and a third drug, typically being a boosted PI, a NNRTI, often called “non-nucs,” and InSTIs such as RAL, EVG, DTG, or BIC. Many of these drugs are available in fixed-dose combinations as well as increasing numbers of drugs as single-tablet regimens.
When should antiviral therapy be started for Human Immunodeficiency Virus or HIV?
There are similar guidelines for treatment throughout the World for treatment. All guidelines recommend starting ART as soon as a person is diagnosed with HIV regardless of CD4 cell count and presence of symptoms.
Evidence for this in part comes from HPTN 052 study, demonstrating that amongst couples where one person is HIV-infected and the other is not, those who were on antiretroviral therapy were 96% less likely to transmit HIV to their uninfected partner than those not on treatment. This was further supported by observational studies (PARTNERS 1, PARTNERS 2 and Opposites Attract) showing that those with plasma viral load < 200-400 copies/mL who had condomless sex with their uninfected partners were not observed to transmit HIV. Finally, a large study was recently reported that demonstrated unequivocally that starting therapy even with a CD4 cell count of greater than 500 cells/mm3 was associated with less risk of disease progression than waiting until CD4 cells were less than 350 cells/mm3.
Before starting treatment, patients must be aware of the short- and long-term side effects of the allopathic drugs, including the fact that some long-term complications may not be known.
Nucleoside and nucleotide analogue reverse transcriptase inhibitors (NRTIs)
NRTIs block an enzyme of the human immunodeficiency virus called reverse transcriptase that allows HIV to infect human cells, particularly CD4 cells or lymphocytes. Reverse transcriptase converts HIV genetic material (RNA) into human genetic material (DNA). The human-like DNA of HIV then becomes part of the infected person’s own cells, allowing the cell to produce RNA copies of the HIV that can then go on to attack other not yet infected cells. Thus, blocking reverse transcriptase prevents HIV from taking over (infecting) human cells. 
In general, most antiviral regimens for HIV disease contain a backbone of at least two NRTIs. The NRTIs include zidovudine (Retrovir, ZDV), stavudine (Zerit, d4T), didanosine (Videx, ddI), zalcitabine (HIVID, ddC), lamivudine (Epivir, 3TC), emtricitabine (Emtriva, FTC), abacavir (Ziagen, ABC), tenofovir disoproxil fumarate (Viread, TDF), and tenofovir alafenamide (Descovy, TAF).
That said, many combinations of NRTIs can be used together, with current guidelines generally recommending the fixed-dose combination of TDF with FTC (Truvada), or TAF with FTC (Descovy), both of which are also available as part of single tablet regimens. An alternative regimen uses the fixed-dose combination of ABC/3TC (Epzicom) alone or combined as a single tablet regimen with DTG (Triumeq).
ABC has been associated with severe allergic reactions in approximately 5% of patients. Recent studies have shown that a blood test (HLA-B*5701) can be performed to determine who is at risk for this reaction so that the drug can be avoided in these individuals and be used in others with greater confidence that there will not be such a reaction. In fact, when available, it is now the standard of care to perform this test prior to initiation of ABC. The main side effects associated with TDF are reduced kidney function and bone density.
What are the usual dosing schedule and meal restrictions for NRTIs?
| ZDV | d4T | ddI | ddC | 3TC | ABC | TDF | TAF | FTC | |
| ZDV, zidovudine; d4T, stavudine; ddI, didanosine; ddC, zalcitabine; 3TC, lamivudine; ABC, abacavir; TDF, tenofovir disoproxil fumarate; TAF, tenofovir alafenamide; FTC, emtricitabine.
*Dosed at 10mg when combined in single tablet regimen with EVG/COBI/FTC/TAF |
|||||||||
| Dose in each pill (mg) | 300 | 30 or 40 | 100 or 400 | 0.75 | 150 or 300 | 300 | 300 | 25* | 200 |
| Schedule | 1 twice a day | 1 twice a day | 2 (100) twice a day or 1 (400) once a day |
1 thrice a day | 1 (150) twice a day or 1 (300) once a day | 1 twice a day or 2 once a day | 1 once a day | 1 once a day | 1 once a day |
| Meal restrictions | None | None | 30 minutes before or 60 minutes after a meal | None | None | None | None | None | None |
The following are available fixed-dose combination pills of NRTIs:
- ZDV/3TC (300 mg/150 mg) as Combivir; one twice per day
- ZDV/3TC/ABC (300 mg/150 mg/300 mg) as Trizivir; one twice per day
- ABC/3TC (600 mg/300 mg) as Epzicom; one per day
- TDF/FTC (300 mg/200 mg) as Truvada; one per day
- TAF/FTC (25 mg/200 mg) as Descovy; one per day
These are standard doses for average-sized adults, and dosing may vary depending upon the weight of a patient. Certain combinations of drugs in this class should generally be avoided, including d4T with ZDV or ddI, 3TC with FTC, and TDF with ddI.
The new formulation of tenofovir (TAF) is available as combination pills only, including EVG/COBI/FTC/TAF (Genvoya, 150/150/200/10 mg), FTC/TAF (Descovy, 200/25 mg), TAF/FTC/RPV (Odefsey, 25/200/25 mg), BIC/FTC/TAF (25/200/25 mg), and darunavir (DRV)/Cobicistat (COBI)/FTC/TAF (800/150/200/10 mg). The new formulation of tenofovir results in lower plasma levels and higher intracellular concentrations of the active drug. Data demonstrate that compared to TDF-containing regimens this form is equally effective with less adverse effects on bone mineral density and possibly on the kidneys.
Non-nucleoside analogue reverse transcriptase inhibitors (NNRTIs)
Like NRTIs, NNRTIs block the reverse transcriptase enzyme, preventing uninfected cells from becoming infected.
NNRTIs include nevirapine (NVP), delavirdine (DLV), efavirenz (EFV), etravirine (ETR), rilpivirine (RPV), and doravirine (DOR). ETR was developed specifically to be an option for patients who have developed resistance to the earlier drugs in the class. NVP, DLV, EFV, RPV, and DOR are typically used with two NRTIs, and ETR is primarily being used as part of regimens for those with a history of different types of treatment to which they have developed resistance.
Table
| Usual dosing schedule and meal restrictions for NNRTIs | ||||||
| NVP | DLV | EFV | ETR | RPV | DOR | |
| NVP, nevirapine; DLV, delavirdine; EFV, efavirenz; ETR, etravirine; RPV, rilpivirine; DOR, doravirine.
*A new formulation is available for dosing as one 400 mg tablet (Viramune XR) once a day. |
||||||
| Dose in each pill (mg) |
200 | 200 | 600 | 200 | 50 | 100 |
| Schedule | 1 twice a day (Start with 1 once a day for first 14 days) |
2 thrice/day | 1 once a day | 1 twice a day | 1 once a day | 1 once a day |
| Meal restrictions | None | None | Avoid high-fat meals | After meals | with meals | None |
*Efavirenz is available as part of fixed-dose combination with lamivudine and tenofovir disoproxil fumarate at a dose of 400 mg (Symfi Lo).
Dosage
For people without a history of drug resistance, there are now several effective fixed-dose combination pills that include TDF plus FTC with either EFV (Atripla) or TDF plus 3TC with EFV (Symfi [using EFV 600 mg] or Symfi Lo [using EFV 400 mg]). TDF with FTC is combined with RPV (Complera), or TDF plus 3TC with DOR (Delstrigo), all of which are available as a single pill that can be taken once per day. There is also a formulation of TAF plus FTC with RPV (Odefsey). 
The combination with RPV was shown to be very effective and well tolerated but not as good at suppressing the viral load as the combination with EFV (Atripla), particularly amongst those who started therapy with higher viral loads and lower CD4 cell counts (for example, >100,000 copies/mL and <200 cells/mm3, respectively). It is currently recommended only for those that have viral load levels of <100,000 copies/mL and CD4 cell counts greater than 200 cells/mm3.
What are protease inhibitors?
PIs block the action of an HIV enzyme called protease that allows HIV to produce infectious copies of itself within HIV-infected human cells. Thus, blocking protease prevents HIV in already-infected cells from producing HIV that can infect other, not yet infected cells.
PIs includes
- saquinavir (Invirase and Fortovase, SQV), which comes as the hard gel capsule Invirase (INV),
- ritonavir (Norvir, RTV),
- indinavir (Crixivan, IDV),
- nelfinavir (Viracept, NFV),
- fosamprenavir (Lexiva, FPV),
- lopinavir/ritonavir (Kaletra, LPV/r),
- atazanavir (Reyataz, ATV), and
- tipranavir (Aptivus, TPV),
- darunavir (Prezista, DRV).
Each of these drugs has been shown to effectively reduce the viral load when used in combination with other active drugs.
LPV
LPV/r comes coformulated as Kaletra while all other RTV-containing regimens require taking RTV along with the other PI. In the case of TPV, RTV must be given as 200 mg with each dose of TPV twice per day. In contrast, ATV can be given without RTV at a dose of two 200 mg capsules once daily or 300 mg with 100 mg RTV once daily. The latter should always be used in PI-experienced subjects and when used in combination with TDF or NNRTIs which can reduce the drug levels of ATV. Similarly, FPV is also used differently in PI-naïve and experienced individuals.
Dosage
In treatment-naïve individuals, it can be given as two 700 mg tablets twice daily or two 700 mg tablets (1,400 mg total) with either 100 or 200 mg RTV, all once daily. In treatment-experienced patients, or when used with NNRTIs, it should be given as one 700 mg tablet with 100 mg RTV, both twice daily. The most recently approved of the PIs is DRV, which was initially used exclusively in treatment-experienced patients with drug-resistant virus. In this setting, it is given as 600 mg with 100 mg RTV, both given twice daily. More recently, DRV was approved for those who have never been treated before given at a dose of 800 mg once daily with 100 mg of RTV once daily.
Table
| Usual dosing schedule and meal restrictions for PIs | ||||||||
| SQV+ | IDV | NFV | FPV | LPV/r | ATV | TPV | DRV | |
| SQV, saquinavir; IDV, indinavir; NFV, nelfinavir; FPV, fosamprenavir; LPV/r, lopinavir plus ritonavir; ATV, atazanavir; TPV, tipranavir; DRV, darunavir.
Administered with RTV at a dose of 100 mg twice a day. FPV can be given without RTV in patients without resistance to PIs or at a dose of 1,400 mg once daily with either 100 mg or 200 mg of RTV once daily. In treatment-experienced patients, FPV is given at a dose of 700 mg twice daily with RTV 100 mg twice daily. ATV can be given alone at a dose of 400 mg once daily or at a dose of 300 mg once daily with RTV 100 mg or COBI 150 mg once/daily. TPV is always given at a dose of 500 mg twice/daily with RTV 200 mg twice daily. DRV can be given to those with a history of drug resistance at a dose of 600 mg twice daily with 100 mg RTV twice daily. For those without resistance, it can be given at a dose of 800 mg with 100 mg RTV or 150 mg COBI once daily. |
||||||||
| Dose in each pill (mg) | 500 | 400 | 625 | 700 | 200/50 | 200 or 300 | 250 | 400 or 600 |
| Schedule | 21 twice a day | 2 every 8 hours | 2 twice a day | 2 twice a day or with RTV2 | 2 twice a day or 4 once a day | 2 (200) or 1 (300) with RTV or COBI3 once a day | 24 twice a day | 8005 once a day with RTV or COBI given once per day or 600 twice a day with RTV given with each dose5 |
| Meal restrictions | with large meals | 1 hour before or 2 hours after meals, or with low-fat meals | with meals | None | With meals | with meals | with meals | with meals |
Side effects
Although RTV is approved for treatment of HIV-infected patients at a dose of 600 mg twice daily, it is virtually never used at this dose because of severe side effects. Because of this, it is not included in the above table. However, PIs are frequently dosed with low doses of RTV. RTV delays the clearance of the other drugs from the system, making them easier to take and more effective. The dose of RTV varies depending upon which drugs it is being taken with and how it is being administered. The only PI that is not substantially affected by RTV is NFV.
COBI
Another recently approved boosting agent is COBI which has no anti-HIV activity but can be given with once daily ATV or DRV as an alternative to RTV for pharmacologic boosting. There are also fixed-dose combinations of each, for example, ATV 300 mg combined with COBI 150 mg (Evotaz) and DRV 800 mg combined with COBI 150 mg (Prezcobix). A single-tablet formulation is now also available with DRV/COBI/FTC/TAF (800/150/200/10 mg) once daily.
What are fusion inhibitors?
A fusion inhibitor blocks an early step in the viral life cycle. Enfuvirtide (Fuzeon, T-20) attaches to the 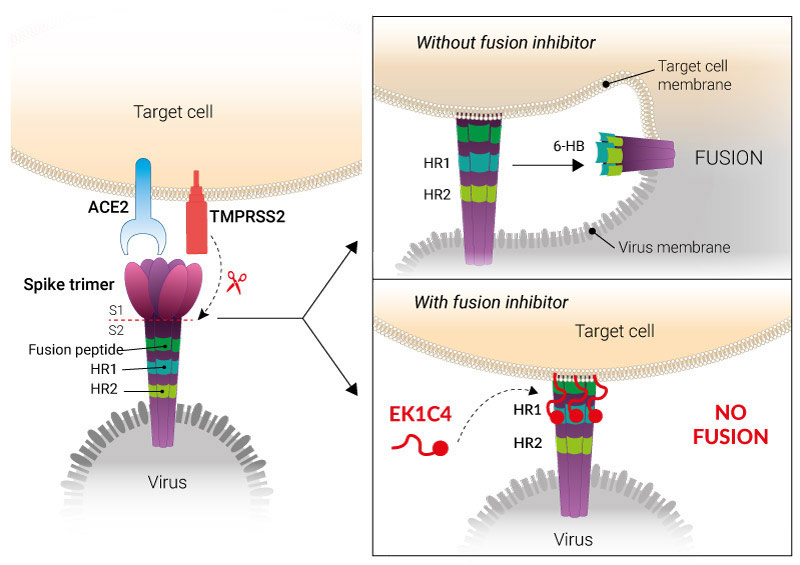 envelope surrounding the virus and prevents it from entering the CD4 cells. This prevents the infection of CD4 cells by HIV. T-20 is the first approved drug in this class. It is given as a twice-daily subcutaneous injection (90 mg). It is used primarily in individuals who have developed resistance to other classes of drugs in order to create a new potent combination. Like all other antivirals, it is most useful in those taking other active drugs at the same time in order to optimize the chance of getting viral loads to undetectable levels and to prevent the development of drug resistance.
envelope surrounding the virus and prevents it from entering the CD4 cells. This prevents the infection of CD4 cells by HIV. T-20 is the first approved drug in this class. It is given as a twice-daily subcutaneous injection (90 mg). It is used primarily in individuals who have developed resistance to other classes of drugs in order to create a new potent combination. Like all other antivirals, it is most useful in those taking other active drugs at the same time in order to optimize the chance of getting viral loads to undetectable levels and to prevent the development of drug resistance.
What is a CCR5 antagonist?
The only available drug in this class is called maraviroc (Selzentry, MVC), which is now approved for use in combination therapy in treatment-experienced and naïve patients who do not have detectable CXCR4-using virus as determined by a tropism assay. This is a unique drug in a new class that blocks viral entry by interacting with the CCR5 molecule on the surface of the CD4 cell. It is known that HIV first binds to the CD4 molecule on the surface of CD4 cells and then connects with the CCR5 or CXCR4 molecule. Only after this second step is the virus able to enter the cell. The CCR5 antagonist prevents viruses that use CCR5 from getting into the cell.
What is unique about this drug compared to others is that 20%-50% of patients have viruses that are able to use the CXCR4 receptor. In these cases, CCR5 antagonists do not appear to be active at suppressing virus. Therefore, in order to know if the drug will work for a given patient, a new test needs to be performed, the so-called tropism assays. This test will tell the provider and patient whether there is virus that uses CXCR4, in which case the patient would not be a candidate for MVC, or if they only have viruses that use CCR5, in which case MVC should be an active drug. Without tropism results, it is impossible to know whether MVC will be an active drug for a given patient.
MVC dose
MVC is typically dosed at either 300 mg or 150 mg twice daily, depending upon what other drugs it is given with. If the patient is taking any RTV, then they would usually receive the 150 mg dose. If RTV is not being used as part of the regimen, they would generally receive the 300 mg dose and sometimes even higher if it is being used with drugs like ETR. HIV providers are aware that whenever using any anti-HIV medications attention must be given to possible drug interactions.
What is an integrase strand transfer inhibitor?
The first available drug in this class was RAL, which is very potent at suppressing HIV in all patients who have never been on this drug or others in the class. It was initially approved for treatment-experienced patients with drug-resistant virus. It is also now approved for those starting therapy for the first time. The approved dose of RAL is 400 mg twice daily with a newer formulation that can be given to those starting therapy for the first time or stably suppressed on RAL twice daily that can be given as two 600 mg tablets once daily.
The second drug
As noted above, a second drug in this class, EVG, is approved for use as first-line therapy as part of the fixed-dose combination pill of TDF/FTC/COBI/EVG and more recently TAF/FTC/COBI/EVG as a stand-alone drug for use in treatment-experienced patients combining it with a ritonavir-boosted PI. This drug is well tolerated and given as one pill per day, but unlike RAL it does need to be taken with food, and it has interactions with other drugs since it must be used with RTV or COBI, so it must be used with caution in those on multiple medications.
Thethireddrug
Another InSTI, DTG is currently recommended for those starting therapy for the first time with either TDF/FTC or ABC/3TC and is available as a fixed-dose combination of ABC/3TC/DTG that can be given as a single pill per day. This drug has a limited number of drug-drug interactions and is generally well tolerated with resistance rarely emerging in those experience virologic failure. It is also frequently active in those who have developed InSTI resistance to RAL and EVG, although it often needs to be given in this setting at a dose of 50 mg twice daily.
Lates research
The most recently approved InSTI is called bictegravir (BIC) that has few drug-drug interactions, is potent, well-tolerated, and can be given with or without food. It is only available as a single-tablet regimen as BIC/FTC/TAF. Thus far, data suggests that selection of drug resistance in those starting therapy with this regimen is extremely rare.
| Usual dosing schedule and meal restrictions for InSTIs | ||||
| RAL | EVG1 | DTG | BIC2 | |
| RAL, raltegravir; EVG, elvitegravir; DTG, dolutegravir; BIC, bictegravir. 1Currently, it is approved as part of the fixed-dose combination pill of EVG (150 mg)/COBI (150 mg)/FTC (200 mg) with either TDF (300 mg) or TAF (25 mg). 2DTG must be given twice per day in patients with history of InSTI resistance. BIC is only available at single-tablet regimen BIC (50 mg)/FTC (200 mg)/TAF (10 mg). 3Available at dose of 600 mg tablet given as two pills once daily for those starting therapy for first time or stably suppressed on a regimen with 400 mg given twice daily. | ||||
| Dose in each pill (mg) | 4003 | 150 | 502 | 50 |
| Schedule | 1 twice a day | 1 per day | 1 per day | 1 per day |
| Meal restrictions | None | With food | None | None |
Two large studies recently demonstrated that in those with viral loads less than 500,000 copies/mL a regimen of DTG plus 3TC was as effective in suppressing viral after one year as the traditional regimen of DTG with two NRTIs. This regimen will likely soon be available as a single-tablet regimen for initial therapy in those without chronic hepatitis B, no underlying drug resistance, and viral loads less than 500,000 copies/mL.
Combination drugs
There are now 10 approved combination pills that allow for a full regimen to be taken as a single pill once per day, so called single tablet regimens. This includes the following NRTI plus third drug combinations:
- TDF/FTC/EFV (300/200/600 mg) as Atripla,
- TDF/3TC/EFV (300/300/600 mg) as Symfi,
- TDF/3TC/EFV (300/300/400 mg) as Symfi Lo,
- TDF/FTC/RPV (300/200/25 mg) as Complera,
- TAF/FTC/RPV (25/200/25 mg) as Odefsey,
- TDF/FTC/EVG/COBI (300/200/150/150 mg) as Stribild,
- TAF/FTC/EVG/COBI (25/200/150/150 mg) as Genvoya,
- ABC/3TC/DTG (600/300/50 mg) as Triumeq,
- 3TC/DTG (300/50 mg) as Dovato,
- BIC/FTC/TAF (50/200/10) as Biktarvy,
- DRV/COBI/FTC/TAF (800/150/200/10) as Symtuza,
- DOR/3TC/TDF (100/300/300) as Delstrigo,
- DTG/RPV (50/25) as Juluca, which is only approved for those stably suppressed on an alternative regimen with no history of drug resistance.
What is an entry inhibitor?
A monoclonal antibody called ibalizumab (Trogarzo) binds the CD4 molecule (a receptor for HIV on cells), which prevents viral entry into the cell. Medical professionals administer the drug as an intravenous infusion of 2,000 mg once, then two weeks later at 2,000 mg again, followed by 800 mg every two weeks. It is appropriate for heavily treatment-experienced patients with multidrug resistant virus who need new therapeutic options in order to achieve an undetectable viral load.
A small molecule oral agent called fostemsavir (Rukobia) is a prodrug of temsavir that binds gp120 on the surface of HIV and prevents viral entry into the cell. The drug is given at a dose of 600 mg twice daily. It is currently approved for those heavily treatment-experienced with multidrug resistant virus who need new therapeutic options in order to achieve an undetectable viral load.
What happens if the patient’s viral load increases while on allopathic therapy?
If the patient does suppress their virus to undetectable levels on antiviral allopathic therapy but then  develops detectable virus, several things should be considered. First, it must be established that the patient is taking the medications correctly. If they are missing doses, then every effort must be made to understand why this is happening and correct the situation, if possible.
develops detectable virus, several things should be considered. First, it must be established that the patient is taking the medications correctly. If they are missing doses, then every effort must be made to understand why this is happening and correct the situation, if possible.
But if the poor adherence is a result of drug side effects, efforts should be directed toward managing the side effects or changing to a better-tolerated regimen. If poor adherence is occurring because of the medication schedule of dosing, new strategies should be discussed such as placing medications in a pillbox, associating the dosing with certain daily activities such as tooth brushing, or possibly changing the regimen. Finally, if the reason for poor adherence is depression, substance abuse, or another personal issue, these issues need to be addressed and managed.
Unexpected increase
It is important to remember that sometimes, for reasons not entirely understood, the viral load can briefly increase. Unexpected increases, therefore, necessitate repeated testing of the viral load before any clinical decisions are made. If, however, the viral load is continually detected despite proper adherence to the prescribed therapy, serious consideration must be given to the possibility that the virus has become resistant to one or more of the medications being given, especially if viral load is greater than 200 copies/mL. There is now an abundance of data showing that the use of drug-resistance tests can improve the response to a follow-up regimen.
Testing can be used to determine if an individual’s HIV has become resistant to one or more of the drugs that are being taken. There are currently two main types of resistance tests available in the clinic: one that is called a genotype and the other a phenotype assay. The former looks for mutations in the virus and the latter the actual amount of drug it takes to block infection by the patient’s virus. The genotype test is very helpful in those being screened for the presence of resistant virus prior to initiating treatment and those experiencing viral rebound on one of their first treatment regimens. The phenotype test is particularly useful in those who are highly treatment experienced and have substantial amounts of drug resistance, especially to the protease class.
Final result
The information derived from these tests, along with a tropism test will ultimately tell the provider which of the many approved drugs are likely to be fully active against the specific patient’s virus. Using this information, the goal is to include at least two and at times preferably three fully active drugs in the next regimen in order to optimize the chances of suppressing the viral load to undetectable levels. It is often useful to seek expert consultation in managing those with multidrug resistant virus.
Allopathic treatment for Human Immunodeficiency Virus during pregnancy
One of the greatest advances in the allopathic management of HIV infection has been in pregnant women. Prior to allopathic antiviral therapy, the risk of HIV transmission from an infected mother to her newborn was approximately 25%-35%. The first major advance in this area came with studies giving ZDV after the first trimester of pregnancy, then intravenously during the delivery process, and then after delivery to the newborn for six weeks.
This treatment showed a reduction in the risk of transmission to less than 10%. There is strong data that women who have viral suppression during pregnancy have a very low risk of transmitting HIV to their baby, perhaps even less than 1%. Current recommendations are to advise HIV-infected pregnant women regarding both the unknown side effects of antiviral therapy on the fetus and the promising clinical experience with potent therapy in preventing transmission. In the final analysis, however, pregnant women with HIV should be treated essentially the same as nonpregnant women with HIV. The choice of medications in this situation should be determined after consultation with an expert in treating HIV-infected pregnant women.
Obstetric precautions
All HIV-infected pregnant women should be managed by an obstetrician with experience in dealing with HIV-infected women. Maximal obstetric precautions to minimize transmission of the HIV virus, such as avoiding scalp monitors and minimizing labor after rupture of the uterine membranes, should be observed. In addition, the potential use of an elective Caesarean section (C-section) should be discussed, particularly in those women without good viral control of their HIV infection where the risk of transmission may be increased. Breastfeeding should be avoided if alternative nutrition for the infant is available since HIV transmission can occur by this route. When breastfeeding is done, it should be in conjunction with antiretroviral therapy for the mother if at all possible.
What can be done for patients who have severe immunosuppression?
Although one goal of antiviral therapy is to prevent the development of immune suppression, some individuals are already immunosuppressed when they first seek medical care. In addition, others may progress to that stage as a result of resistance to antiviral drugs. Nevertheless, every effort must be made to optimize antiviral therapy in these patients. In addition, certain specific antibiotics should be initiated, depending on the number of CD4 cells, to prevent the complications (that is, the opportunistic infections) that are associated with HIV immunosuppression. Guidelines for the prevention of opportunistic infections can be found at https://aidsinfo.nih.gov/
Preventive treatment
In summary, patients with a CD4 cell count of less than 200 cells/mm3 should receive preventative treatment against Pneumocystis jiroveci with trimethoprim/sulfamethoxazole, given once daily or three times weekly. If they are intolerant to that drug, patients can be treated with an alternative drug such as dapsone or atovaquone. Those patients with a CD4 cell count of less than 100 cells/mm3 who also have evidence of past infection with Toxoplasma gondii, which is usually determined by the presence of Toxoplasma antibodies in the blood, should receive trimethoprim/sulfamethoxazole. Toxoplasmosis is an opportunistic parasitic disease that affects the brain and liver. If a person is using dapsone to prevent Pneumocystis jiroveci, pyrimethamine and leucovorin can be added once a week to dapsone to prevent toxoplasmosis.
Finally, patients with a CD4 cell count of less than 50 cells/mm3 that are not planning to start suppressive antiretroviral therapy in the near future should receive preventive treatment for Mycobacterium avium complex (MAC) infection with weekly azithromycin, or as an alternative, twice daily clarithromycin or rifabutin. MAC is an opportunistic bacterium that causes infection throughout the body. Many of these drugs can be stopped if initial antiviral therapy results in good viral suppression and sustained increases in CD4 cells.
Homeopathic Treatment for Human Immunodeficiency Virus or HIV
No single remedy can cure a person with HIV or AIDS completely; I (Dr Qaisar Ahmed) always advise few medicines (combination) according to each and every patient’s individual history.
These homeopathic medications can be used in conjunction with antiretroviral therapy (ART) along with other treatments for Human Immunodeficiency Virus and/or AIDS and have been shown to be very effective in alleviating some of the commonly encountered symptoms and complications.
But utmost care must be ensured and these homeopathic medicine for HIV positive patients should not be taken without consulting a homeopathic doctor.
Homeopathic medicines for HIV are:
Syphilinum
Abscess; succession of abscesses. Alcoholism; hereditary craving for alcohol. Anus, fissure of. Aphasia. :max_bytes(150000):strip_icc()/maculopapular-569fdede3df78cafda9eb2dd.png) Asthma. Breasts sensitive. Bubo. Constipation. Crying of infants. Deafness. Deltoid rheumatism. Dentition. Diplopia. Dysmenorrhea. Epilepsy. Headache; syphilitic. Hoarseness; before menses. Iritis. Leucorrhea; infantile. Mouth, ulcerated. Myopia. Neuralgia. Human Immunodeficiency Virus. AIDS. Night-sweats. Ophthalmia. Otorrhea. Ovaries, affections of. Ozena. Pemphigus. Psoas abscess. Ptosis. Rectum, stricture of. Rheumatism. Sciatica. Sleeplessness. Spine, caries of. Strabismus. Stricture. Sunstroke. Syphilis. Teeth, carious. Throat, ulcerated. Tibia, pains in. Tongue, cracked, ulcerated. Ulcers. Whitlow.
Asthma. Breasts sensitive. Bubo. Constipation. Crying of infants. Deafness. Deltoid rheumatism. Dentition. Diplopia. Dysmenorrhea. Epilepsy. Headache; syphilitic. Hoarseness; before menses. Iritis. Leucorrhea; infantile. Mouth, ulcerated. Myopia. Neuralgia. Human Immunodeficiency Virus. AIDS. Night-sweats. Ophthalmia. Otorrhea. Ovaries, affections of. Ozena. Pemphigus. Psoas abscess. Ptosis. Rectum, stricture of. Rheumatism. Sciatica. Sleeplessness. Spine, caries of. Strabismus. Stricture. Sunstroke. Syphilis. Teeth, carious. Throat, ulcerated. Tibia, pains in. Tongue, cracked, ulcerated. Ulcers. Whitlow.
Crotalus Horridus
Amblyopia. Apoplexy. Appendicitis. Bilious fever. Boils. Cancers. Carbuncles. Cerebro-spinal meningitis. Chancre. Ciliary neuralgia. Convulsions. Delirium tremens. Dementia. Diphtheria. Dysmenorrhea. Dyspepsia. Ears, discharges from. Ecchymosis. Epilepsy. Eyes affections. Erysipelas. Hematuria. Hemorrhagic diathesis. Headache. Heart affections. Herpes. Human Immunodeficiency Virus. AIDS. Hydrophobia. Intestinal hemorrhage. Jaundice. Keratitis. Liver diseases. Lung’s affections. Mastitis. Measles. Milk-leg. Meningitis. Ovaries affections. Ozaena. Palpitation. Peritonitis. Peri typhlitis. Phlebitis. Psoriasis palmaris. Purpura. Pyemia. Remittent fever. Rheumatism. Scarlatina. Sleeplessness. Tongue, inflammation, cancers. Ulcers. Urticaria. Vaccination side effects.
Arsenicum Album
Abscess. Acne rosacea. Alcoholism. Amenorrhea. Anemia. Aphthae. Cancer, oral cancers. Carbuncle. Delirium tremens. Dropsy. Dyspepsia. Eczema. Endometritis. Enteric fever. Epithelioma. Erysipelas. Fainting. Fever. Gangrene. Gastric ulcer. Gastritis. Glandular swellings. Gout. Herpes zoster. Human Immunodeficiency Virus. AIDS. Hodgkin’s disease. Hydrothorax. Hypochondriasis. Ichthyosis. Jaundice. Kidney diseases. Leucorrhea. Lupus. Malignant pustule. Nails diseased. Nettle-rash. Neuralgia. Neuritis. Pityriasis. Plethora. Pleurisy. Pleurodynia. Pneumonia. Psoriasis. Immune thrombocytopenic purpura. Pyemia. Pyelitis. Remittent fever. Rheumatic gout. Rheumatism. Thirst. Yellow fever.
Arsenicum Iodatum
Acne rosacea Aneurysm. Angina pectoris. Breast, tumor of. Bronchitis. Cancer. AIDS. HIV. Catarrh. Consumption. Debility. Dropsy. Epithelioma. Gastritis. Hay-fever. Heart affections. Hydrothorax. Laryngitis. Leucocythemia. Lichen. Liver affections. Lung’s affections. Measles. Otorrhea. Pneumonia. Rheumatism. Scrofulous ophthalmia. Syphilis.
Mercurius Solubilis
Abscess. Anemia. Aphthae. Appendicitis. Balanitis. Bone, disease of. Brain inflammation. Breath, 
Mercurius Corrosive
Antrum of Highmore affections. Aphthae. Appendicitis. Bones diseases. Bright’s disease. Cancers. Chancre. Human Immunodeficiency Virus, AIDS. Diarrhea. Dysentery. Eczema. Enteric fever. Gums affections. Intestines, ulcerated. Intussusception. Iritis. Jaundice. Kidney’s inflammation. Labour, puerperal fever. Miscarriage. Esophagus strictures. Paralysis. Paraphimosis. Pemphigus. Peri metritis, Peritonitis. Prosoplasia. Rigg’s disease. Supraorbital neuralgia. Syphilis. Tabes mesenterica. Taste disordered. Tenesmus.
Thuja Occidentalis
Abdomen, distended. Abortion. Angina pectoris. Anus, fistula in; fissure of. Asthma. Balanitis. Cancer. Catalepsy. Chorea. Clavus. Condylomas. Constipation. Convulsions. Coxalgia. Diarrhea. Dyspareunia. Dysmenorrhea. Ear polypus. Enuresis. Epilepsy. Epulis. Eyes tumors; granular inflammation. Fatty tumors. Feet, fetid. Flatus, incarcerated. Frontal sinuses, catarrh of. Ganglion. Gleet. Gonorrhea. Hemorrhage. Hemorrhoids. Hair affections. HIV. AIDS. Herpes zoster. Ichthyosis. Intussusception. Jaws, growth on. Joints, cracking in. Levitation. Morvan’s disease. Mucous patches. Muscae volitantes. Myopia. Naevus. Neuralgia. Paralysis. Pemphigus. Polypus. Post-nasal catarrh. Pregnancy, imaginary. Prostate disease. Ptosis. Ranula. Rheumatism, gonorrheal. Rickets. Teeth caries. Tongue ulcers; biting of. Tumors. Vaccination side effects. Vaginismus. Warts.
Fagonia Arabica or Dhamasa
A best anti-viral of a unique kind of action with brilliant results. Various kinds of cancers (breast cancer, liver cancer, anal cancer, and lung cancer etc). Hepatitis A, B, and C. Infections. AIDS. Human Immunodeficiency Virus.
Sulphur
Acne. AIDS. Adenoids. Ague. Amaurosis. Amenorrhea. Anemia. Bedsores. Biliousness. Boils. Brain congestion. Breasts affections. Bright’s disease. Chronic bronchitis. Chagres fever. Chancre. Cheloid. Constipation. Consumption. Corns. Cough. Dental fistula. Diabetes. Diarrhea. Dysentery. Dysmenorrhea. Ear affections. Eczema. Emaciation. Enuresis. Fever. Freckles. Ganglion. Gland’s affections. Gout. Hemorrhoids. Human Immunodeficiency Virus. Herpes. Jaundice. Laryngitis. Leucorrhea. Lichen. Liver derangement. Lumbago. Lung’s affections. Lupus. Mania. Miscarriage. Esophageal constriction. Ophthalmia, acute; scrofulous; rheumatic. Pelvic hematocele. Phimosis. Peritonitis. Pneumonia. Skin affections. Smell illusions. Spinal irritation, curvature. Spleen diseases. Ulcers. Warts. White swelling. Worms.
Silica Tera
Abdomen distended. Abscess. AIDS. Acne. Anemia. Anal fissure; fistula. Boils. Bones necrosis. Cancer.  Carbuncle. Cellulitis. Cheloid. Constipation. Debility. Diabetes. Elephantiasis. Enchondroma. Enuresis. Eruptions. Excrescences. Fibroma. Glandular swellings. Human Immunodeficiency Virus. Jaw caries. Joints – synovitis. Lachrymal fistula. Locomotor ataxy. Mania. Morvan’s disease. Nails diseases. Necrosis. Neuralgia, Spinal irritation. Strains. Strangury. Nodes. Perspiration offensive. Phimosis. Pleurisy. Prepuce eruption. Psoas abscess. Pylorus suppuration. Rheumatism; chronic; hereditary. Suppuration. Teeth caries. Tenesmus. Tumors. Ulcers. Urethral stricture. Urine incontinence. Vaccination side effects. Vaginal spasms. Worms.
Carbuncle. Cellulitis. Cheloid. Constipation. Debility. Diabetes. Elephantiasis. Enchondroma. Enuresis. Eruptions. Excrescences. Fibroma. Glandular swellings. Human Immunodeficiency Virus. Jaw caries. Joints – synovitis. Lachrymal fistula. Locomotor ataxy. Mania. Morvan’s disease. Nails diseases. Necrosis. Neuralgia, Spinal irritation. Strains. Strangury. Nodes. Perspiration offensive. Phimosis. Pleurisy. Prepuce eruption. Psoas abscess. Pylorus suppuration. Rheumatism; chronic; hereditary. Suppuration. Teeth caries. Tenesmus. Tumors. Ulcers. Urethral stricture. Urine incontinence. Vaccination side effects. Vaginal spasms. Worms.
Tuberculinum
Acne. AIDS. Albuminuria. Appendicitis. Asthma. Bones, caries of. Bronchitis. Catarrhal pneumonia. Chilblains. Cornea, opacity of; ulceration of. Dentition. Erysipelas. Erythema. Hematuria. Hemoptysis. Headache. Heart affections; palpitation of. Human Immunodeficiency Virus. Influenza. Leprosy. Leucorrhea. Lung’s edema. Lupus. Mania. Menses too early. Nephritis. Night-terrors. Edema glottidis. Paralysis. Phthisis. Pleurisy. Pneumonia, acute. Tuberculosis.
Kali carbonicum for Human Immunodeficiency Virus or HIV
Amenorrhea. AIDS. Anemia. Biliousness. Bronchitis. Catarrh. Consumption. Cough. Debility. Dropsy. Dysmenorrhea. Dyspepsia. Ear inflammation. Eyes inflammation; oedema around. Face blotches. Gastralgia. Hemorrhage. Hemorrhoids. Heart affections. Hip-joint disease. Human Immunodeficiency Virus. Hydrothorax. Hysteria. Kidney’s infections. Knee infections; white leg/white swelling. Larynx catarrh. Leucorrhea. Liver infections. Lumbago. Menorrhagia. Metrorrhagia. Pleurisy. Pleurodynia. Proctalgia. Urticaria. Uterine cancers.
Bacillinum
Addison’s disease. Alopecia. Consumptiveness Growth, defective. Hydrocephalus. Idiocy. Insanity. Joints affections. Pityriasis Ringworm. Scrofulous glands. Teeth, defective; pitted. Tuberculosis. Human Immunodeficiency Virus.
Phosphorus
AIDS. Alopecia areata. Amaurosis. Anemia, acute pernicious. Anal fissure. Human Immunodeficiency Virus. Arteries inflammations. Bones diseases, cancers. Brain infections; softening. Breast abscess; fistulae. Bronchitis; membranous. Chlorosis. Chorea. Ciliary neuralgia. Coccygodynia. Constipation. Consumption. Corpulency. Diarrhea. Dropsy. Ecchymosis. Erotomania. Fainting. Fatty degeneration. Fungus haematoidin. Gums ulceration. Hematuria. Hemorrhagic diathesis. Heart degeneration; murmurs. Jaundice; malignant; of pregnancy. Joints affections. Lactation disorders. Liver diseases; acute yellow atrophy. Locomotor ataxy. Lumps, hemorrhage from; edema; paralysis. Marasmus. Menorrhagia. Nails ulcers. Neuralgia. Nosal bleedings.
Odor of body, changed. Esophageal pain. Ozaena. Pancreatic diseases. Paralysis; pseudo-hypertrophic; general of insane. Periostitis. Perspiration abnormal. Pneumonia. Proctalgia. Proctitis. Progressive muscular atrophy. Pruritus ani. Psoriasis. Puerperal convulsions. Immune thrombocytopenic purpura. Pylorus, thickening of. Rheumatism; paralytic. Shivering. Spine curvature. Syringomyelia. Tumors; erectile; polypoid; cancerous. Ulcers. Urethra stricture. Yellow fever.
Petroleum
Petroleum acts on sweat and oil glands, symptoms worse during the winter season. AIDS. Addison’s disease. Albuminuria. Anemia. Angina pectoris. Anal fissure. Bedsores. Breath offensive. Burns. Chilblains. Chlorosis. Constipation. Cracks in skin. Deafness. Diarrhea. Dyspepsia. Eczema. Herpes. Herpes preputial. Human Immunodeficiency Virus. Irritation. Perspiration offensive. Presbyopia. Prostatitis. Psoriasis. Rheumatism. Urethral stricture; chronic inflammation. Varices. Vomiting. Warts.
Nitric Acidium
Actinomycosis. AIDS. Anus, fissure of. Axilla, offensive perspiration of. Bladder, chronic catarrh of. Breath, offensive. Bright’s disease. Bronchitis. Bubo. Chancre. Cheloid. Chilblains. Constipation.  Dysentery. Dyspepsia. Glandular swellings. Hematuria. Hemorrhages. Herpes. Human Immunodeficiency Virus. In growing toenail. Mouth, sore. Mucous patches. Muscae volitantes. Myopia. Nails affections. Paralysis. Perspiration, abnormal. Phimosis. Polypus. Proctitis. Prostate suppuration. Salivation. Taste disordered. Tongue, ulcers. Ulcers. Warts. Wens.
Dysentery. Dyspepsia. Glandular swellings. Hematuria. Hemorrhages. Herpes. Human Immunodeficiency Virus. In growing toenail. Mouth, sore. Mucous patches. Muscae volitantes. Myopia. Nails affections. Paralysis. Perspiration, abnormal. Phimosis. Polypus. Proctitis. Prostate suppuration. Salivation. Taste disordered. Tongue, ulcers. Ulcers. Warts. Wens.
Swelling, inflammation of prepuce, and phimosis. Paraphimosis. Ulcers, like Cancers (after Mercury; especially with exuberant granulations), on prepuce and glans (with pricking, stinging pains).
Deep, fistulous, irregular, ragged ulcers on the glans, with elevated, lead-colored, extremely sensitive edges. Red, scurfy spots on the corona glands. Inflammatory swelling of testes. Violent stitches in vagina. Excoriations in vulva between thighs, Ulcer, with burning itching in vagina. Excrescences on vaginal portion of uterus as large as lentils; great voluptuousness of mucous membrane in genitals after coitus. Uterine hemorrhages from overexertion of body.
Sepia
Amenorrhea. Ascarides. Cancer. Chorea. Condylomas. Cystitis. Dyspepsia. Eczema. Epistaxis. Eyes affections. Face yellow. Herpes circinate. Jaundice. Leucorrhea. Liver-spots. Liver, torpid. Menstruation, disordered. Mind, affections of. Nails pains. Neuralgia. Nose inflamed; swollen. Ozaena. Phimosis. Pityriasis versicolor. Pleurisy. Psoriasis. Ptosis. Rectal cancer; fissure. Ringworm. Sacrum, pain in. Urine incontinence. Uterus – bearing down sensation. Varicose veins. Warts.
Sarsaparilla for Human Immunodeficiency Virus or HIV
Herpes and offensive sweat about genitals; the skin lies in folds Asthma. Bladder affections. Bones affections. Breast scirrhous. Bright’s disease. Climaxes. Constipation. Dyspepsia. Dysuria. Enuresis. Eruptions. Eyes affections. Faintness. Gland’s enlargement. Gout. Herpes – of prepuce. Plica polonica. Renal colic. Rhagades. Rheumatism; gonorrheal. Seborrhoea. Spermatic cords swelling. Spermatorrhea. Strangury. Ulcers. Warts. Human Immunodeficiency Virus. AIDS. Intolerable stench on genitals. Herpetic eruption on genitals. Itching on scrotum and perineum.
Natrum muriaticum
Addison’s disease. AIDS. Anemia. Aphthae. Atrophy. Brain-fag. Catarrh. Chorea. Constipation. Debility. Depression. Diabetes. Dyspareunia. Dropsy. Dyspepsia. Goiter. Gonorrhea. Gout. Heart affections. Hemiopia. Herpes, herpes circinate. Hodgkin’s disease. Hypochondriasis. Human Immunodeficiency Virus. Leucocythemia. Leucorrhea. Lung’s edema. Mouth inflammation. Nettle rash. Pediculosis. Ranula. Seborrhoea. Spinal irritation. Splenomegaly. Stomatitis. Taste lost; disordered. Tongue blistered; white coated; heavy. Trifacial-nerve paralysis. Ulcers. Varices. Vaginismus. Vertigo. Warts. Strong fetid odor from genital organs. Hydrocele.
Graphites
Acne. AIDS. Anal affections. Breasts, indurated, cancer. Cancer. Catarrh. Chaps. Chlorosis. Colic. Constipation. Deafness. Dropsy. Dysmenorrhea. Ears affections. Eczema. Epistaxis. Erysipelas. Fissures. Gastralgia. Glandular swellings. Gleet. Gravel. Hemorrhoids. Herpes. Human Immunodeficiency Virus. Liver indurated. Nails disorders, infections. Obesity. Ovarian tumors. Paralysis. Parotitis. Psoriasis. Ptosis. Smell disorders. Tumors. Ulcers. Urine disordered. Uterus cancer. Vaccination side effects. Worms.
Hepar Sulphuricum
Abscess. AIDS. Amaurosis. Angina pectoris. Appetite, disordered. Asthma. Axilla, abscess in. Beard, eruptions of. Blepharitis. Boils. Breast, affections of. Bronchitis. Bubo. Burns. Carbuncle. Caries.  Chilblains. Chlorosis. Cold. Constipation. Consumption. Cornea, ulceration of; opacity of. Cough. Croup. Diarrhea. Eczema. Emphysema. Erysipelas. Glandular swellings. Hemorrhoids. Herpes preputial. Human Immunodeficiency Virus. Jaundice. Joints affections. Laryngitis. Leucorrhea. Lupus. Marasmus. Menorrhagia. Mouth sore. Ovaries affections. Pneumonia. Rheumatism. Skin affections. Spinal irritation. Urticaria. Wens.
Chilblains. Chlorosis. Cold. Constipation. Consumption. Cornea, ulceration of; opacity of. Cough. Croup. Diarrhea. Eczema. Emphysema. Erysipelas. Glandular swellings. Hemorrhoids. Herpes preputial. Human Immunodeficiency Virus. Jaundice. Joints affections. Laryngitis. Leucorrhea. Lupus. Marasmus. Menorrhagia. Mouth sore. Ovaries affections. Pneumonia. Rheumatism. Skin affections. Spinal irritation. Urticaria. Wens.
Herpes, sensitive, bleed easily. Ulcers externally on prepuce similar to chancre. Suppurating inguinal glands. Figworts with offensive odor. Humid soreness on genitals and between scrotum and thigh. Obstinate gonorrhea.
Discharge of blood from uterus. Itching of pudenda and nipples, worse during menses. Abscesses of labia with great sensitiveness.
Kreosotum
Acne. AIDS. Amenorrhea. Cancer. Carbuncle. Constipation. Consumption. Diarrhea. Ear affections. Enuresis. Epithelioma. Gastralia. Hemorrhagic diathesis. Herpes. Hysterical vomiting. Human Immunodeficiency Virus. Leucorrhea. Lip epithelioma. Lupus. Neuralgia. Ovary affections. Prostate. Rheumatism. Teeth caries. Ulcers. Urine incontinence. Burning in genitals (during coition) and impotence. Prepuce bluish black with hemorrhages and gangrene.
Shootings in vagina, as if produced by electricity. Voluptuous itching in vagina. Itching in vagina, inducing rubbing in evening, succeeded by smarting, swelling, heat, and induration of external parts, with soreness in vagina when urinating.
Medorrhinum
AIDS. Asthma. Clonic spasms. Corns. Diabetes. Dysmenorrhea. Epilepsy. Eyes inflammation. Favus. Gleet. Gonorrhea, suppressed. Gonorrheal rheumatism. Human Immunodeficiency Virus. Liver abscess. Masturbation. Ovaries pains. Pelvic cellulitis. Polypi. Priapism. Psoriasis palmaris. Ptosis. Renal colic. Rheumatism. Sciatica. Shoulder, pains in. Stricture. Urticaria. Warts. Suppressed gonorrhea.
Variolinum
Exanthema of sharp, pointed pimples. AIDS. Human Immunodeficiency Virus. Petechial eruptions. Shingles. Enlargement of testicle. Hard swelling of testicle.
Var. 1m in a spoon of water every day for HIV.
Alumen
The clinical application of this remedy points to its bowel symptoms, both in obstinate constipation and in hemorrhage from bowels in the course of typhoid-one phase of the paralytic weakness of the muscles in all parts of the body. Human Immunodeficiency Virus. AIDS, tendency to induration is also marked, a low form of tissue-making is favored. Hardening of tissues of tongue, rectum, uterus, etc; ulcers with indurated base. Adapted to old people, especially bronchial catarrhs. Sensation of dryness and constriction. Mental paresis; dysphagia especially to liquids. Tendency to induration, Scirrhous of the tongue.
P. S: This article is only for doctors having good knowledge about Homeopathy and allopathy, for learning purpose(s).
For proper consultation and treatment, please visit our clinic.
None of above-mentioned medicine(s) is/are the full/complete treatment but just hints for treatment; every patient has his/her own constitutional medicine.
 Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Senior research officer at Dnepropetrovsk state medical academy Ukraine.
Location: Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Find more about Dr Sayed Qaisar Ahmed at:
https://www.youtube.com/Dr Qaisar Ahmed
https://www.facebook.com/ahmed drqaisar
https://www.drqaisarahmed.com.