
These uterine fibroids are noncancerous growths of the uterus that often appear during childbearing years. Also called leiomyomas (lie-o-my-O-muhs) or myomas, uterine fibroids aren’t associated with an increased risk of uterine cancer and almost never develop into cancer.
Myomas, and leiomyomas are commonly seen in women during the reproductive years between the ages of 16 and 50.
Hormones are thought to play a big factor in the development of fibroids, as they occur in the presence of high estrogen levels and naturally begin to shrink during menopause when estrogen levels drop. Genetics, obesity, and vascular system problems also have an association with some fibroid cases. Fibroids are also common in women who have never borne children or began their menstrual cycle before the age of 10 years old.
Fibroids range in size from seedlings, undetectable by the human eye, to bulky masses that can distort and enlarge the uterus. A patient can have a single fibroid or multiple ones. In extreme cases, multiple fibroids can expand the uterus so much that it reaches the rib cage and can add weight.
Symptoms
In almost all cases, fibroids don’t have any symptoms, in those that do, can be influenced by the location, size and number of fibroids.
The most common signs and symptoms of uterine fibroids include:
- Heavy menstrual bleeding,
- Menstrual periods lasting more than a week,
- Pelvic pressure or pain,
- Frequent urination,
- Difficulty emptying the bladder,
- Constipation,
- Backache or leg pains.
Rarely, a uterine fibroid can cause acute pain when it outgrows its blood supply, and begins to die.
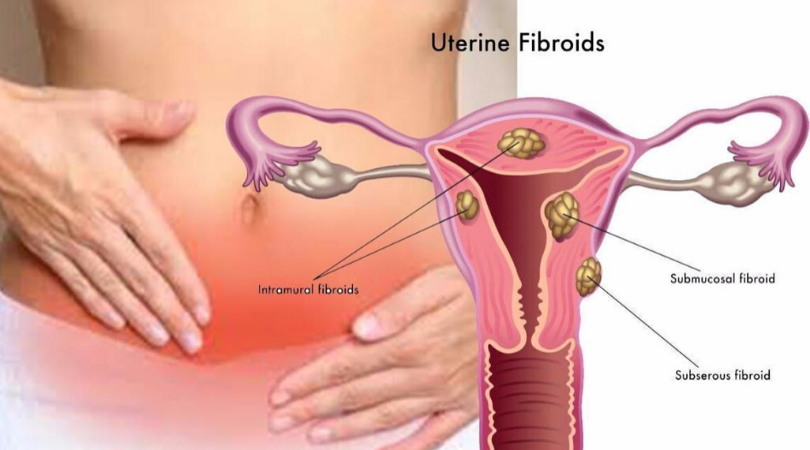
Uterine fibroids are generally classified by their location. Intramural fibroids grow within the muscular uterine wall. Submucosal fibroids bulge into the uterine cavity. Subserosal fibroids project to the outside of the uterus.
Symptoms
See your doctor if you have:
- Pelvic pain that doesn’t go away,
- Overly heavy, prolonged or painful periods,
- Spotting or bleeding between periods,
- Difficulty emptying your bladder,
- Unexplained low red blood cell count (anemia).
Lady should seek prompt medical care if she has severe vaginal bleeding or sharp pelvic pain that comes on suddenly.
Causes of Uterine Fibroids
Researchers still don’t know the cause of uterine fibroids, but research and clinical experience point to these factors:
- Genetic changes. Many fibroids contain changes in genes that differ from those in typical uterine muscle cells.
- Hormones. Estrogen and progesterone, two hormones that stimulate development of the uterine lining during each menstrual cycle in preparation for pregnancy, appear to promote the growth of fibroids. Uterine fibroids contain more estrogen and progesterone receptors than typical uterine muscle cells do. Uterine fibroids tend to shrink after menopause due to a decrease in hormone production.
- Other growth factors. Allopathic drugs that help the body maintain tissues, such as insulin-like growth factor, may affect fibroid growth.
- Extracellular matrix (ECM). ECM is the material that makes cells stick together, like mortar between bricks. ECM is increased in fibroids and makes them fibrous. ECM also stores growth factors and causes biologic changes in the cells themselves.
Doctors believe that uterine fibroids develop from a stem cell in the smooth muscular tissue of the uterus (myometrium). A single cell divides repeatedly, eventually creating a firm, rubbery mass distinct from nearby tissue.
The growth patterns of uterine fibroids vary — they may grow slowly or rapidly, or they may remain the same size. Some fibroids go through growth spurts, and some may shrink on their own.
Many fibroids that have been present during pregnancy shrink or disappear after pregnancy, as the uterus goes back to its usual size.
Risk factors of Fibroids
There are few known risk factors for uterine fibroids, other than being a woman of reproductive age. Factors that can have an impact on fibroid development include:
- Race. Although all women of reproductive age could develop fibroids, black women are more likely to have fibroids than are women of other racial groups. In addition, black women have fibroids at younger ages, and they’re also likely to have more or larger fibroids, along with more-severe symptoms.
- Heredity. If your mother or sister had fibroids, you’re at increased risk of developing them.
- Other factors. Starting the periods at an early age; obesity; a vitamin D deficiency; having a diet higher in process food (canned/bottled), inorganic food, white sugar, fast food, broiler chickens, carbonated drinks, alcoholism etc and lower in green vegetables.
Complications
Some doctors hinks that uterine fibroids usually aren’t dangerous, but I (Dr Qaisar Ahmed) think that any abnormality in organism can prevent to dangerous/fatal diseases, can cause discomfort and may lead to complications such as a drop in red blood cells (anemia), which causes fatigue, from heavy blood loss therefore could be treated as soon a possible.
Pregnancy and uterine fibroids
Uterine fibroids usually don’t interfere with getting pregnant. However, it’s possible that fibroids — especially submucosal fibroids — could cause infertility or pregnancy loss.
Uterine fibroids may also raise the risk of certain pregnancy complications, such as placental abruption, fetal growth restriction and preterm delivery.
Diagnosis
Uterine fibroids are frequently found incidentally during a routine pelvic exam. A doctor may feel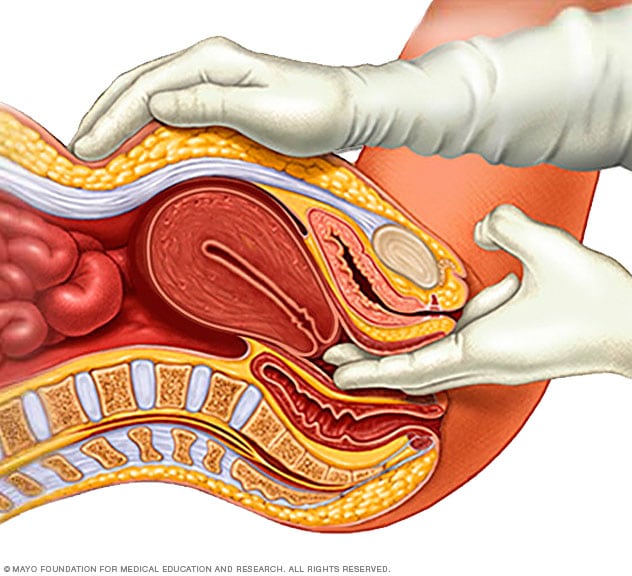 irregularities in the shape of uterus, suggesting the presence of fibroids.
irregularities in the shape of uterus, suggesting the presence of fibroids.
If patient has symptoms of uterine fibroids, a doctor may order these tests:
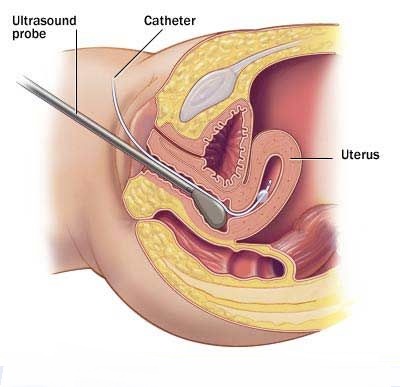
- Ultrasound. A doctor or technician moves the ultrasound device (transducer) over the patient’s abdomen (transabdominal) or places it inside the vagina (transvaginal) to get images of your uterus.
- Lab tests. If you have abnormal menstrual bleeding, your doctor may order other tests to investigate potential causes. These might include a complete blood count (CBC) to determine if you have anemia because of chronic blood loss and other blood tests to rule out bleeding disorders or thyroid problems.
Other imaging tests
- Magnetic resonance imaging (MRI). This imaging test can show in more detail the size and location of fibroids, identify different types of tumors, and help determine appropriate treatment options. An MRI is most often used in women with a larger uterus or in women approaching menopause (perimenopause).
- Hysterosonography. Hysterosonography (his-tur-o-suh-NOG-ruh-fee), also called a saline infusion sonogram, uses sterile salt water (saline) to expand the uterine cavity, making it easier to get images of submucosal fibroids and the lining of the uterus in women attempting pregnancy or who have heavy menstrual bleeding.
- Hysterosalpingography. Hysterosalpingography (his-tur-o-sal-ping-GOG-ruh-fee) uses a dye to highlight the uterine cavity and fallopian tubes on X-ray images. Your doctor may recommend it if infertility is a concern. This test can help your doctor determine if your fallopian tubes are open or are blocked and can show some submucosal fibroids.
- Hysteroscopy. For this exam, your doctor inserts a small, lighted telescope called a hysteroscope through your cervix into your uterus. Your doctor then injects saline into your uterus, expanding the uterine cavity and allowing your doctor to examine the walls of your uterus and the openings of your fallopian tubes.
Traditional fibroid treatment involves the removal of the uterus in a hysterectomy procedure or heavy dosages of medication to dissolve the benign, smooth muscle masses. Either option has severe consequences during the childbearing years, but now there are less invasive procedures and more natural ways.
Allopathic Treatment for uterine fibroids
Traditional allopathic fibroid treatment involves the removal of the uterus (hysterectomy) or heavy dosages of drugs to dissolve the benign, smooth muscle masses. Either option has severe consequences during the childbearing years, but now there are less invasive procedures and more natural medicated ways for example Homeopathy.
Allopathic drugs for uterine fibroids target hormones that regulate menstrual cycle, treating symptoms such as heavy menstrual bleeding and pelvic pressure. But they don’t eliminate uterine fibroids, but may shrink them. Medications include:
Gonadotropin-releasing hormone (GnRH) agonists
Medications called GnRH agonists treat fibroids by blocking the production of estrogen and progesterone, putting patient into a temporary menopause-like state. As a result, menstruation stops, fibroids shrink and anemia often improves. GnRH agonists include leuprolide (Lupron Depot, Eligard, others), goserelin (Zoladex) and triptorelin (Trelstar, Triptodur Kit). Many women have significant hot flashes while using GnRH agonists. GnRH agonists typically are used for no more than three to six months because symptoms return when the medication is stopped and long-term use can cause loss of bone (osteoporosis). A doctor may prescribe a GnRH agonist to shrink the size of uterine fibroids before a planned surgery or to help transition to menopause.
Progestin-releasing intrauterine device (IUD)
A progestin-releasing IUD can relieve heavy bleeding caused by uterine fibroids. A progestin-releasing IUD provides symptom relief only and doesn’t shrink fibroids or make them disappear. It also prevents pregnancy.
Tranexamic acid (Lysteda, Cyklokapron)
This non hormonal medication is taken to ease heavy menstrual periods. It’s taken only on heavy bleeding days.
Other medications
A doctor might recommend other medications for example, oral contraceptives can help control menstrual bleeding, but they don’t reduce fibroid size. Nonsteroidal anti-inflammatory drugs (NSAIDs), which are not hormonal medications, may be effective in relieving pain related to fibroids, but they don’t reduce bleeding caused by fibroids. A doctor may also suggest that his patient vitamins and iron if patient has heavy menstrual bleeding and anemia.
Allopathic Noninvasive procedure
- A noninvasive treatment option for uterine fibroids that preserves patient’s uterus, requires no incision and is done on an outpatient basis.
- Performed while patient is inside an MRI scanner equipped with a high-energy ultrasound transducer for treatment. The images gives us the precise location of the uterine fibroids. When the location of the fibroid is targeted, the ultrasound transducer focuses sound waves (sonications) into the fibroid to heat and destroy small areas of fibroid tissue.
- Newer technology, so allopathic researchers are still learning more about the long-term safety and effectiveness.
Minimally invasive procedures
 Certain procedures can destroy uterine fibroids without actually removing them through surgery. They include:
Certain procedures can destroy uterine fibroids without actually removing them through surgery. They include:
Uterine artery embolization
Small particles (embolic agents) are injected into the arteries supplying the uterus, cutting off blood flow to fibroids, causing them to shrink and die. This technique can be effective in shrinking fibroids and relieving the symptoms they cause. Complications may occur if the blood supply to the ovaries or other organs is compromised. However, research shows that complications are similar to surgical fibroid treatments.
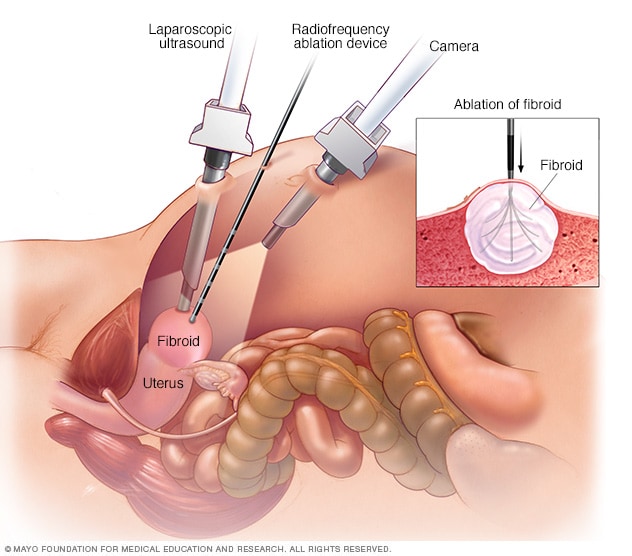
Radiofrequency ablation
In this procedure, radiofrequency energy destroys uterine fibroids and shrinks the blood vessels that feed them. This can be done during a laparoscopic or transcervical procedure. A similar procedure called cryomyolysis freezes the fibroids.With laparoscopic radiofrequency ablation (Acessa), also called Lap-RFA, doctor makes two small incisions in the abdomen to insert laparoscope, using the laparoscopic camera and a laparoscopic ultrasound tool, doctor locates fibroids to be treated.
After locating a fibroid, doctor uses a specialized device to deploy several small needles into the fibroid. The needles heat up the fibroid tissue, destroying it. The destroyed fibroid immediately changes consistency, for instance from being hard like a golf ball to being soft like a marshmallow. During the next three to 12 months, the fibroid continues to shrink, improving symptoms.
Because there’s no cutting of uterine tissue, doctors consider Lap-RFA a less invasive alternative to hysterectomy and myomectomy. Most women who have the procedure get back to regular activities after 5 to 7 days of recovery.
The transcervical — or through the cervix — approach to radiofrequency ablation (Sonata) also uses ultrasound guidance to locate fibroids.
Laparoscopic or robotic myomectomy
In a myomectomy, surgeon removes the fibroids, leaving the uterus in place. If the fibroids are few in number, doctor may opt for a laparoscopic or robotic procedure, which uses slender instruments inserted through small incisions in patient’s abdomen to remove the fibroids from uterus. Larger fibroids can be removed through smaller incisions by breaking them into pieces (morcellation), which can be done inside a surgical bag, or by extending one incision to remove the fibroids. Robotic myomectomy gives surgeon a magnified, 3D view of the uterus, offering more precision, flexibility and dexterity than is possible using some other techniques.
If the fibroids are few in number, doctor may opt for a laparoscopic or robotic procedure, which uses slender instruments inserted through small incisions in patient’s abdomen to remove the fibroids from uterus. Larger fibroids can be removed through smaller incisions by breaking them into pieces (morcellation), which can be done inside a surgical bag, or by extending one incision to remove the fibroids. Robotic myomectomy gives surgeon a magnified, 3D view of the uterus, offering more precision, flexibility and dexterity than is possible using some other techniques.
Hysteroscopic myomectomy
This procedure may be an option if the fibroids are contained inside the uterus (submucosal). The surgeon accesses and removes fibroids using instruments inserted through the vagina and cervix into the uterus.
Endometrial ablation
This treatment, performed with a specialized instrument inserted into the uterus, uses heat, microwave energy, hot water or electric current to destroy the lining of the uterus, either ending menstruation or reducing patient’s menstrual flow.
Typically, endometrial ablation is effective in stopping abnormal bleeding. Submucosal fibroids can be removed at the time of hysteroscopy for endometrial ablation, but this doesn’t affect fibroids outside the interior lining of the uterus. Women aren’t likely to get pregnant following endometrial ablation, but birth control is needed to prevent a pregnancy from developing ectopic pregnancy.
With any procedure that doesn’t remove the uterus, there’s a risk that new fibroids could grow and cause symptoms.
Traditional allopathic surgical procedures
Options for traditional surgical procedures include:
- Abdominal myomectomy. If patient has multiple fibroids, very large fibroids or very deep fibroids, the doctor may use an open abdominal surgical procedure to remove the fibroids. Many women who are told that hysterectomy is their only option can have an abdominal myomectomy instead. However, scarring after surgery can affect future fertility.
- Hysterectomy. This surgery removes the uterus. It remains the only proven permanent solution for uterine fibroids. Hysterectomy ends patient’s ability to bear children, the surgery brings on menopause and the question of whether the patient will take hormone replacement therapy. Sometimes a women with uterine fibroids may be able to choose to keep their ovaries.
Morcellation during fibroid removal
Morcellation — a process of breaking fibroids into smaller pieces — may increase the risk of spreading cancer if a previously undiagnosed cancerous mass undergoes morcellation during myomectomy. There are several ways to reduce that risk, such as evaluating risk factors before surgery, morcellating the fibroid in a bag or expanding an incision to avoid morcellation.
All myomectomies carry the risk of cutting into an undiagnosed cancer, but younger, premenopausal women generally have a lower risk of undiagnosed cancer than do older women.
Also, complications during open surgery are more common than the chance of spreading an undiagnosed cancer in a fibroid during a minimally invasive procedure.
I (Dr qaisar Ahmed) categorically against the use of a device to morcellate the tissue (power morcellator) for most women having fibroids removed through myomectomy or hysterectomy. In particular, the women who are approaching menopause or who have reached menopause avoid power morcellation. Older women in or entering menopause may have a higher cancer risk, and women who are no longer concerned about preserving their fertility have additional treatment options for uterine fibroids.
Risk of developing new uterine fibroids after allopathic treatment 
For all procedures except hysterectomy, seedlings — tiny tumors that the doctor doesn’t detect during surgery — could eventually grow and cause symptoms that warrant treatment. This is often termed the recurrence rate. New fibroids, which may or may not require treatment, also can develop.
Also, some procedures — such as laparoscopic or robotic myomectomy, radiofrequency ablation, or MRI-guided focused ultrasound surgery (FUS) — may only treat some of the fibroids present at the time of treatment.
Homeopathic Treatment for Uterine Fibroids
Many women who are told that hysterectomy is their only option can chose the Homeopathic treatment instead. Homeopathy treats and cures the uterine fibroids and co-diseases or abnormalities’.
Here are few of well proven Homeopathic medicines:
Terebinthina
Catamenia retarded and scanty. Drawing in thighs and colic as if menses would set in, a week after she had had them. Uterus and ovaries very painful. Ovarian dropsy. Terrible burning in uterus, with great bearing-down pain; caused great heat all over; craves drink; inward heat. Uterine diseases after wearing pessaries. Fibroids; bloody leucorrhoea; burning in uterus; menorrhagia, black blood. Herpes labialis. Abortion. Neuralgia during pregnancy. Burning and bearing down in uterus during urination. Metritis, lochia checked, burning in uterus. Peritonitis after confinement from tight-lacing.
Alumen
A low form of tissue-making is favored, paralytic weakness of the muscles in all parts of the body. Tendency to induration. Hardening of tissues of uterus. Uterine fibroids. Tendency to induration of neck of uterus and mammary glands. Chronic yellow vaginal discharge. Chronic gonorrhoea, yellow, with little lumps along urethra. Aphthous patches in vagina. Menses watery.
Caulophyllum Thalictroides
This is a woman’s remedy. Want of tonicity of the womb. Extraordinary rigidity of os. Uterine fibroids. Spasmodic and severe pains, which radiates in all directions; shivering, without progress; false pains. Revives labor pains and furthers progress of labor. After pains. Leucorrhoea, with moth-spots on forehead. Habitual abortion from uterine debility. Needle-like pains in cervix. Dysmenorrhoea, with pains radiates to other parts of body. Lochia protracted; great atony. Menses and leucorrhoea profuse.
Conium Maculatum
Dysmenorrhoea, with drawing-down thighs. Uterine fibroids. Menses delayed and scanty; parts sensitive. Breasts enlarge and become painful before and during menses. Rash before menses. Itching around pudenda. Unready conception. Induration of os and cervix. Ovaritis; ovary enlarged, indurated; lancinating pain. Ill effects of repressed sexual desire or suppressed menses, or from excessive indulgence. Leucorrhoea after micturition. Trouble at the change of life, old and bachelors. Growth of tumors. Cancerous diathesis, scrofulous and cancerous conditions.. Enlarged glands.
Carbo Animalis
Nausea of pregnancy; worse at night. Lochia offensive. Menses too early, frequent long lasting, followed by great exhaustion, so weak, can hardly speak, flow only in morning. Burning in vagina and labia. Darting in breast; painful indurations in breast. Cancer of uterus, burning pain down thighs.
Secale Cornutum

Produces contraction of the unstriped muscular fibers; hence a constringent feeling throughout the whole body. Anaemic, coldness, numbness, petechiae, mortification, gangrene. Uterine fibroids. Menstrual colic, with coldness and intolerance of heat. Passive haemorrhages in feeble, cachectic women. Burning uterine pains. Brownish, offensive leucorrhoea. Menses irregular, copious, dark; continuous oozing of watery blood until next period. Threatened abortion about the third month.
A useful remedy for shriveled skin-thin, scrawny women. Haemorrhages; continued oozing; thin, fetid, watery black blood. Debility, anxiety, emaciation, though appetite and thirst may be excessive. Facial and abdominal muscles twitch.
Belladonna
Belladonna has a marked action on the vascular system, skin and glands. Sensitive forcing downwards, as if all the viscera would protrude at genitals. Dryness and heat of vagina. Dragging around loins. Pain in sacrum. Menses increased; bright red, too early, too profuse. Haemorrhage hot. Cutting pain from hip to hip. Uterine fibroids. Mastitis pain, throbbing, redness, streaks radiate from nipple. Breasts feel heavy; are hard and red. Tumors of breast, pain worse lying down. Badly smelling haemorrhages, hot gushes of blood. Diminished lochia.
Cocculus Indicus
Dysmenorrhoea, with profuse dark menses. Too early menses, clotted, with spasmodic colic. Painful pressing in uterine region, followed by haemorrhoids. Purulent, gushing leucorrhoea between menses; very weakening, can scarcely speak. So weak during menstruation, scarcely able to stand. Uterine fibroids.
Coccus Cacti
Menses too early, profuse, black and thick; dark clots, with dysuria. Intermittent menstruation; flow only in evening and at night. Large clots escape when passing water. Labia inflamed.
Pulsatilla Pratensis
Amenorrhoea. Suppressed menses from uterine fibroids, or chlorosis. Tardy menses. Too late, scanty, thick, dark, clotted, changeable, intermittent. Chilliness, nausea, downward pressure, painful, flow intermits. Leucorrhoea acrid, burning, creamy. Pain in back; tired feeling. Diarrhoea during or after menses.
Cimicifuga Racemosa
Amenorrhoea. Pain in ovarian region; shoots upward and down anterior surface of thighs. Pain immediately before menses. Menses profuse, dark, coagulated, offensive with backache, nervousness; always irregular. Ovarian neuralgia. Pain across pelvis, from hip to hip. After-pains, with great sensitiveness and intolerance to pain. Uterine fibroids. Facial blemishes in young women.
Senecio Aureus
Uterine fibroids. Menses retarded, suppressed. Functional amenorrhoea of young girls with backache. Before menses, inflammatory conditions of throat, chest, and bladder. After menstruation commences, these improve. Anaemic dysmenorrhoea with urinary disturbances. Premature and too profuse menses
Sabadilla 
Menses too late; come by fits and starts, intermit, due to transient and localized congestion of womb alternating with chronic anaemic state, uterine fibroids.
Cantharis Vesicatoria
Retained placenta, with painful urination. Expels moles, tumors, dead foetuses, membranes, etc. Nymphomania. Puerperal metritis, with inflammation of bladder. Menses too early and too profuse; black swelling of vulva with irritation. Constant discharge from uterus. Burning pain in ovaries; extremely sensitive. Pain in os coccyx, lancinating and tearing. Uterine fibroids.
Nitricum Acidum
Uterine fibroids. Leucorrhoea brown, flesh-colored, watery, or stringy, offensive. Hair on genitals falls out (Natr m, Zinc). Uterine haemorrhages. Menses early, profuse, like muddy water, with pain in back, hips and thighs. Stitches through vagina. Metrorrhagia after parturition.
Silica
Menses too early and too feeble, or else too profuse. Increased menses, with paroxysms of icy coldness over whole body. Suppression of the menses. Discharge of blood before proper period; menses too late; protracted; blood acrid. Metrorrhagia. Diarrhoea, before the menses. During the menses, pains in the abdomen, pale appearance of objects, or burning sensation and excoriation in vulva. Itching in the vulva. Pressing-down feeling in vagina. Itching, burning, and soreness in pudenda; during menses.
Discharge of blood from the uterus, while suckling. Abortion. Leucorrhoea, which flows when urinating, or after the menses. Leucorrhoea, like milk, flowing at intervals, and preceded by gripings in umbilical region. Acrid, corrosive leucorrhoea. Inflammation of nipples.
Thlaspi Bursa Pastoris
Uterine fibroids with prolonged menses (10-15 days). Menses appear very frequently. The next menstrual cycle appears even before recovery from the periods has occurred. Menstrual bleeding is profuse, with the presence of large clots. Violent uterine colic. Cramping pain in the uterus during menstruation in uterine fibroids cases.
Helonias
Loss of sexual desire and power with or without sterility. Profound melancholy, deep, undefined depression, with a sensation of soreness and weight in the womb; “a consciousness of a womb”. Aching, dragging weakness in sacral region, with prolapsus; also at climaxis, with marked debility, profound mental gloom. Prolapsus uteri and ulceration of the cervix; discharge constant, dark, badly smelling; flooding on lifting a weight, and on least exertion; great vaginal irritation.
Uterus low down, fundus tilted forwards; the finger passes with difficulty between the os and the rectum. Menses too frequent and profuse in women who are feeble from loss of blood. Flow passive: dark, coagulated, offensive. Leucorrhoea, with atony and anaemia.
Threatened abortion from atonic conditions. Scanty menstrual flow with heaviness, languor, drowsiness, and albuminous urine. Profuse flooding, with serous leucorrhoea, much uterine and ovarian pain; climaxis. Labia and pudendum hot, red, swollen, burning and itching terribly; epidermis every morning falls off in thin, transparent exfoliation.
Mucous surface of labia red, swollen, covered with a curdy deposit, like aphthae. Threatened abortion; habitual abortion. Albuminuria during pregnancy; great weakness, drowsiness.
Calcarea Carb 
Catamenia premature and too copious. Sterility, with catamenia too early, and too profuse. Before the catamenia, mammae swollen and painful, fatigue, headache, disposition to be frightened, colic, and shivering.
During the catamenia, congestion in the head, with internal heat, or cuttings in the abdomen, and cramp-like pain in the lumbar region, or else vertigo, headache, toothache, nausea, colic, and other sufferings.
Suppressed menstruation, with full habit. Miscarriage. Voluptuous sensation in the genital parts, with emission. Flow of blood at a time different from the catamenia. Metrorrhagia. Itching or pressing in the vagina. Shootings in the orifice of the matrix, and pressive pain in the vagina. Prolapsus uteri, with pressure on the parts. Itching in the womb. Inflammation and swelling of the womb, with redness, purulent discharge, and burning pain. Varices in the labia majora. Leucorrhoea before the catamenia. Leucorrhoea, with burning itching, or else like milk, flowing by fits, and during the emission of urine.
Sepia Officinalis
Pelvic organs relaxed. Bearing-down sensation as if everything would escape through vulva, must cross limbs to prevent protrusion, or press against vulva. Leucorrhoea yellow, greenish; with much itching. Menses Too late and scanty, irregular; early and profuse; sharp clutching pains. Violent stitches upward in the vagina, from uterus to umbilicus. Prolapse of uterus and vagina. Morning sickness. Vagina painful, especially on coition.
Thuja Occidentalis
Vagina very sensitive. Warty excrescences on vulva and perineum. Profuse leucorrhoea; thick, greenish. Severe pain in left ovary and left inguinal region. Menses scanty, retarded. Polypi; fleshy excrescences. Ovaritis; worse left side, at every menstrual period. Profuse perspiration before menses.
Ustilago Maydis
Vicarious menstruation. Ovaries burn, pain, swell. Profuse menses after miscarriage; discharge of blood from slightest provocation; bright red; partly clotted. Menorrhagia at climaxis. Oozing of dark blood, clotted, forming long black strings. Uterus hypertrophied. Cervix bleed easily. Postpartum haemorrhage. Profuse lochia.
Berberis Vulgaris
Tardy enjoyment in women, during coition, and often accompanied with incisive or shooting pains. Sensation of burning and excoriation in the vagina, extending to the labia. Pale catamenia, composed of serous blood. Menses, consisting of grey mucus or brown blood. Suppressed menstruation. During the catamenia, pains in the genital parts and in the loins, or violent pains in the head, with sensation of fainting. Catamenia insufficient, with acute drawing pains in the whole body, painful inflation of the abdomen, pain in the loins, shootings in the chest, dejected aspect, with violent pains in the head; or with ill-humour, disgust of life, dejection, smarting pains in the vagina, sensation of burning and excoriation in the anus, and pains in the arms, as far as the shoulders and the nape of the neck.
Sabina Officinalis
In the case of menstrual bleeding with clots in uterine fibroid cases, Sabina Officinalis is a significant medicine. The slightest motion increases menstrual bleeding. Pain from sacrum to pubis is another attending feature. During menses, pain in the uterus may be present that gets better by lying on the back. Uterine pain may extend to the thighs. Other symptoms include foul, acrid, corrosive, yellow leucorrhoea.
Kreosotum
Corrosive itching within vulva, burning and swelling of labia; violent itching between labia and thighs. During menses, difficult hearing; buzzing and roaring; eruption after. Burning and soreness in external and internal parts. Leucorrhoea, yellow, acrid; odor of green corn; worse between periods. Haemorrhage after coition. Menses too early, prolonged. Vomiting of pregnancy, with ptyalism. Menstrual flow intermits; ceases on sitting or walking; reappears on lying down. Pain worse after menses. Lochia offensive; intermits.
Fraxinus Americana
Uterus enlarged, and patulous. Watery, non irritating leucorrhoea. Fibroids with bearing-down sensation, cramping in feet, worse in afternoon and night. Dysmenorrhoea.
Janosia Ashoka
Leucorrhoea, Amenorrhoea, Metrorrhagia, Menorrhagia, Uterine colic, Urinary Tract Infections, Hemorrhoids with obstinate constipation, Reflex headaches arising due to uterine pathology; unilateral, Irritable and thickened bladder, Disturbed sleep with dreams of travelling. Uterine pathology associated with pain along the spine radiating to abdomen and thighs. Gastric complaints such as desire for sweets, also acid things. Thirsty, excessive nausea
Hemorrhoids with obstinate constipation, Reflex headaches arising due to uterine pathology; unilateral, Irritable and thickened bladder, Disturbed sleep with dreams of travelling. Uterine pathology associated with pain along the spine radiating to abdomen and thighs. Gastric complaints such as desire for sweets, also acid things. Thirsty, excessive nausea
Trillium Pendulum and Kali Carbonicum
In uterine fibroid cases with back pain during the menstrual cycle, Trillium Pendulum comes highly recommended. The pain may radiate to the hips from the back during menses. Tight binding of the back and hips provides relief. Menstrual bleeding is bright red and gushing. The slightest movement worsens uterine bleeding. Trillium Pendulum is also indicated for inter-menstrual bleeding every two weeks. Another attending feature is faintness from uterine bleeding. Kali Carbonicum is selected when there is violent back pain during menses. The pain gets better from sitting and pressure. The menstrual flow is also copious.
Erigeron Canadensis
Erigeron Canadensis is a beneficial medicine for treating frequent urination in case of uterine fibroids. In some cases, painful urination may also arise. The attending features are excessive menstrual bleeding which is bright red in colour. Erigeron Canadensis is also used for inter-menstrual bleeding from slight exertion.
Hepar Sulphuricum
Excoriation of the vulva, and between the thighs. Congestion of blood to the uterus. Irritation of ovaries; with swelling; and great sensitiveness. Discharge of blood between the periods, with inflation of the abdomen. Catamenia too long delayed, and diminished. Leucorrhoea, with smarting at the vulva. Cancerous ulcer on the breast, with stinging-burning of the edges, smelling like old cheese. Itching nipples.
China Officinalis and Ferrum Met
Both China Officinalis and Ferrum Met are effective medicines for treating uterine fibroids with heavy bleeding and anaemia. Among them, China Officinalis works best when there is profuse, dark menstrual bleeding, clots in menstrual blood, exhaustion and anaemia. Fainting spells may also arise. Ferrum Met is best used where the symptoms include pale, watery, heavy and prolonged menses leading to anaemia. Menstrual flow worsens from the slightest movement. Lower back pain or abdomen pain during menses may be observed.
Apis Melifestida
Amenorrhoea or menorrhagia. Inflammation, induration, swelling, and dropsy of the ovaries. Weight and pain in either ovarian region. Enlargement of the ovary with pain, Sharp, cutting, stinging pain in the swollen worse during menstruation. Ovarian tumours, with stinging pains like bee-stings.
Metritis, peritonitis, with stinging, thrusting pains. Pressing-down pain in the uterus. Bearing-down, with sensation as before menses. Dropsy of the ovaries; dropsy of the uterus. Menstruation suppressed or diminished, with congestion to the head.
Labour-like, bearing-down pains, followed by dark, bloody mucus. Threatened miscarriage in the early months, with heaviness of the abdomen, restlessness, and yawning. Abortion. Abortion during the early months. Dropsy in the latter part of pregnancy attended with puerperal convulsions. Ulceration and engorgement of os uteri. Large and painful swelling of the labia, with heat and stinging pains. Erysipelatous inflammation of the breasts. Swelling and hardness of the mammae threatening to ulcerate. Scirrhous or open cancer of the mammae, with stinging, burning pains.
Lilium Tigrinum
Menses early, scanty, dark, clotted, offensive; flow only when moving about. Bearing down sensation with urgent desire for stool, as though all organs would escape. Ceases when resting. Congestion of uterus, prolapse, and anteversion. Constant desire to support parts externally. Pain in ovaries and down thighs. Acrid, brown leucorrhoea; smarting in labia. Sexual instinct awakened. Bloated feeling in uterine region. Subinvolution. Pruritus pudendi.
P. S: This article is only for doctors having good knowledge about Homeopathy and allopathy, for learning purpose(s).
For proper consultation and treatment, please visit our clinic.
None of above-mentioned medicine(s) is/are the full/complete treatment, but just hints for treatment; every patient has his/her own constitutional medicines.
 Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Senior research officer at Dnepropetrovsk state medical academy Ukraine.
Location: Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Find more about Dr Sayed Qaisar Ahmed at:
https://www.youtube.com/Dr Qaisar Ahmed
https://www.facebook.com/ahmed drqaisar
I do not even know the way I finished up right here, but I assumed this post used to be great. I don’t know who you are however definitely you’re going to a well-known blogger when you aren’t already 😉 Cheers!
I have been reading out some of your posts and i can claim nice stuff. I will make sure to bookmark your blog.
Greetings I am so excited I found your web site, I really found you by error, while I was researching on Digg for something else, Nonetheless I am here now and would just like to say kudos for a marvelous post and a all round interesting blog (I also love the theme/design), I don抰 have time to read it all at the minute but I have bookmarked it and also included your RSS feeds, so when I have time I will be back to read much more, Please do keep up the excellent job.
Thanks for sharing superb informations. Your site is so cool. I’m impressed by the details that you抳e on this website. It reveals how nicely you understand this subject. Bookmarked this website page, will come back for more articles. You, my pal, ROCK! I found just the information I already searched all over the place and simply couldn’t come across. What a great website.
Have you ever considered about including a little bit more than just your articles? I mean, what you say is fundamental and everything. Nevertheless think of if you added some great graphics or videos to give your posts more, “pop”! Your content is excellent but with pics and video clips, this site could undeniably be one of the greatest in its niche. Superb blog!
Appreciating the hard work you put into your website and detailed information you offer. It’s nice to come across a blog every once in a while that isn’t the same unwanted rehashed material. Excellent read! I’ve bookmarked your site and I’m including your RSS feeds to my Google account.
Everyone loves what you guys are up too. This kind of clever work and reporting! Keep up the terrific works guys I’ve incorporated you guys to my own blogroll.
glad to be one of the visitors on this amazing website : D.
Aw, this was a really nice post. In thought I want to put in writing like this moreover – taking time and actual effort to make an excellent article… however what can I say… I procrastinate alot and in no way seem to get one thing done.
Thanks, I have been searching for info about this subject matter for ages and yours is the best I’ve discovered so far.
An intriguing discussion is worth comment. There’s no doubt that that you ought to write more on this subject, it might not be a taboo matter but usually folks don’t speak about such topics. To the next! Best wishes!!
Your style is unique in comparison to other people I have read stuff from. Thank you for posting when you’ve got the opportunity, Guess I will just bookmark this site.
I could not refrain from commenting. Perfectly written!
Appreciating the commitment you put into your blog and detailed information you present. It’s great to come across a blog every once in a while that isn’t the same outdated rehashed material. Wonderful read! I’ve saved your site and I’m adding your RSS feeds to my Google account.
🥰🌹
Great blog! I am loving it!! Will be back later to read some more. I am bookmarking your feeds also.
You made some clear points there. I did a search on the subject matter and found most guys will agree with your website.
I like what you guys are up also. Such smart work and reporting! Keep up the superb works guys I抳e incorporated you guys to my blogroll. I think it will improve the value of my web site 🙂
Hi there! I know this is kind of off topic but I was wondering if you knew where I could locate a captcha plugin for my comment form? I’m using the same blog platform as yours and I’m having trouble finding one? Thanks a lot!
Just desire to say your article is as astounding. The clarity in your post is just spectacular and i could assume you’re an expert on this subject. Well with your permission allow me to grab your RSS feed to keep updated with forthcoming post. Thanks a million and please continue the enjoyable work.
Wow, wonderful blog layout! How long have you been blogging for? you make blogging look easy. The overall look of your site is great, let alone the content!
As a Newbie, I am constantly browsing online for articles that can be of assistance to me. Thank you
Wonderful work! This is the type of info that should be shared around the internet. Shame on Google for not positioning this post higher! Come on over and visit my website . Thanks =)
I have been absent for a while, but now I remember why I used to love this site. Thanks , I抣l try and check back more frequently. How frequently you update your site?
I think this is one of the most vital information for me. And i am glad reading your article. But want to remark on some general things, The website style is ideal, the articles is really great : D. Good job, cheers
F*ckin?remarkable issues here. I抦 very satisfied to look your post. Thank you a lot and i’m having a look forward to contact you. Will you please drop me a mail?
I haven抰 checked in here for some time since I thought it was getting boring, but the last few posts are great quality so I guess I will add you back to my everyday bloglist. You deserve it my friend 🙂
Oh my goodness! an incredible article dude. Thank you Nevertheless I am experiencing situation with ur rss . Don抰 know why Unable to subscribe to it. Is there anybody getting identical rss drawback? Anybody who knows kindly respond. Thnkx
That is really interesting, You’re an overly professional blogger. I have joined your rss feed and look forward to looking for more of your wonderful post. Also, I’ve shared your web site in my social networks!
Incredible! This blog looks just like my old one! It’s on a totally different subject but it has pretty much the same layout and design. Wonderful choice of colors!
Nice read, I just passed this onto a colleague who was doing some research on that. And he actually bought me lunch because I found it for him smile So let me rephrase that: Thank you for lunch!
Hello There. I found your blog using msn. This is a really well written article. I抣l make sure to bookmark it and return to read more of your useful information. Thanks for the post. I will definitely return.
Hey very nice site!! Man .. Beautiful .. Amazing .. I’ll bookmark your website and take the feeds also厈I am happy to find a lot of useful information here in the post, we need work out more techniques in this regard, thanks for sharing. . . . . .
Thank you for this article. I might also like to state that it can often be hard when you find yourself in school and merely starting out to establish a long credit standing. There are many individuals who are simply trying to survive and have a good or favourable credit history can occasionally be a difficult element to have.
Great weblog here! Also your site lots up very fast! What web host are you the use of? Can I get your associate hyperlink on your host? I desire my site loaded up as quickly as yours lol
Useful info. Fortunate me I discovered your site unintentionally, and I’m stunned why this coincidence didn’t came about in advance! I bookmarked it.