
Leishmaniasis is a “vector-borne” infection, meaning that an insect (Phlebotomus flies or sand fly) from another host or “reservoir” (disease carrier) transmits it. Various animals, including dogs, rats, sloths, cattle, and humans can act as hosts for Leishmania parasites.
Leishmania spreads to people through the bite of over 30 types of Phlebotomus genus of sand flies. These flies are only up to 2 mm long, they make no sound, and their bite can be painless. The females need blood to produce eggs.
Phlebotomine flies that transmit Leishmania live in the warm tropical and subtropical areas of the world.
As climate changes and temperatures shift, tropical diseases are shifting, as well. Health researchers expect human leishmaniasis to follow the spread of Phlebotomus flies into regions of increasing warmth and humidity. Human migration and increasing urban encroachment into rural areas also offer increased opportunities for spread of these organisms.
Intracellular protozoa parasites from the Leishmania genus cause leishmaniasis. The life cycle is relatively simple. Uninfected sand flies acquire the parasite by feeding on infected people or animals. When the sand fly bites a human, it injects small numbers of parasites that mononuclear blood cells rapidly take up. This stage is the promastigote stage. Once inside the human mononuclear cells, the parasite enters the amastigote stage and begins to multiply and infect other cells and tissues. Depending on the species, the parasites may spread via blood and lymph fluid to other body sites, such as the skin or major organs.
Large epidemics of leishmaniasis can occur among people in crowded areas, or when high rates of malnutrition weaken people in affected regions. Generally, dogs and rodents are the reservoir for most species of Leishmania. Humans may become the primary “reservoir” and source of recurrent infection with leishmaniasis, particularly with L. donovani. This is “anthroponotic” transmission.
Types of leishmaniasis
Many species of Leishmania cause leishmaniasis, a very diverse infection described by syndromes according to what part of the body it affects most. 
Several Leishmania species cause three syndromes:
- Visceral (kala-azar),
- Cutaneous,
- Mucocutaneous leishmaniasis.
Each type may occur more commonly in certain parts of the world than others and depends on the species of Leishmania.
It may take weeks to months or even years for symptoms to appear after the infecting bite.
Cutaneous leishmaniasis (CL) is the most common form of leishmaniasis and, as the name implies, the skin is the predominant site of infection.
Some species of Leishmania cause cutaneous leishmaniasis but also spread to the tissues of the face and upper respiratory tract and cause a mucocutaneous form of the disease many years later.
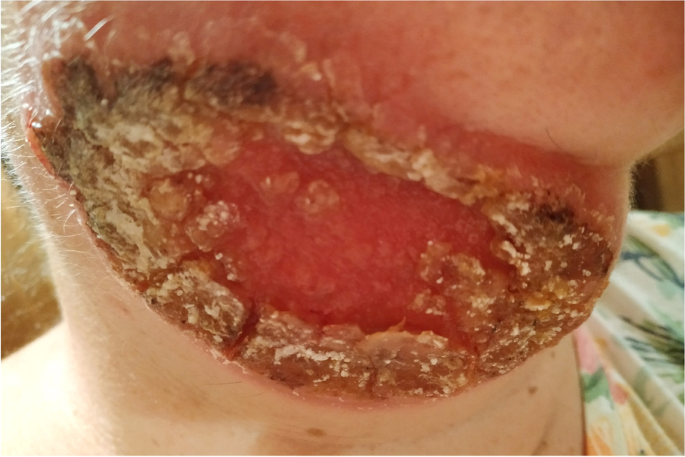
Mucocutaneous leishmaniasis (ML) causes terribly disfiguring and progressive destruction of the nose, nasal septum, mouth, and mid-face. Untreated, death results from secondary infections like pneumonia.
A more severe form of cutaneous leishmaniasis with many lesions, disseminated cutaneous leishmaniasis may occur in people with poor immunity. It may appear very similar to lepromatous leprosy or fungal infection.
In visceral leishmaniasis (VL), the parasite spreads from the skin via the blood and lymph fluids to the vital organs of the body, particularly the liver, spleen, and bone marrow. This type of infection is less common but more life threatening than cutaneous leishmaniasis.
Post-kala azar dermal leishmaniasis occurs in India and Sudan. Skin lesions may appear months to years after apparently healed VL.
Visceral leishmaniasis is also an important yet under-recognized opportunistic infection in HIV-infected people. People with immune suppression due to HIV are double – triple fold more likely to develop severe visceral leishmaniasis, because they lack the cell-mediated immunity needed for defense and recovery from it.
HIV-visceral leishmaniasis co-infection then leads to accelerated progression of HIV infection to advanced disease. Treatment failure and relapse of visceral leishmaniasis is high in these individuals, although anti-retroviral (anti-HIV) therapy helps improve cell-mediated immunity and may have some anti-leishmanial effects as well. Because the parasites multiply in high number, these individuals also become effective human reservoirs, often transmitting both HIV and Leishmania via IV drug use.
Risk factors for leishmaniasis
The major risk factor for leishmaniasis is exposure to infected phlebotomine sand flies. The sand flies are most active from dusk to dawn and are more common in rural areas.

In healthy people, the degree of immune response to leishmaniasis appears to be genetically determined and is primarily cell-mediated; antibodies are not protective.
Cutaneous leishmaniasis lesions in people with normal immunity will resolve without treatment in several weeks. These individuals are immune to cutaneous leishmaniasis thereafter.
In visceral leishmaniasis, a weak cell-mediated immune response is associated with more severe disease. Factors that weaken cell-mediated immunity include malnutrition and co-infection with the human immunodeficiency virus (HIV). The cause of mucocutaneous leishmaniasis remains unclear, but an overactive immune response may play a part.
Interestingly, Leishmania virus can infect the Leishmania parasite itself, which may cause the parasite to be more dangerous by overstimulating the inflammatory response from the human immune system.
Leishmania may live quietly for years in the body and then begin to multiply (reactivate) if the person’s immune system becomes suppressed. For example, people with HIV who are being treated with anti-HIV drugs and whose immunity is improving may develop CL or VL as part of an immune reconstitution syndrome (this refers to hidden infections that reveal themselves as the body begins to fight them).
Thus, people born in a country with leishmaniasis and those who have had travel-related exposure are at risk if they become immunosuppressed by conditions such as chemotherapy, use of steroids, or infection with HIV.
Symptoms
Visceral leishmaniasis (VL) or kala-azar may be mild or severe. Some patients are asymptomatic and do not realize that they carry the parasite. Symptoms appear in weeks to months after the bite of the sand fly. Less commonly, symptoms arise only years later when a person’s immune system becomes suppressed. The five classic findings of more severe disease are:
- Weight loss, which may be severe,
- Low blood counts (pancytopenia),
- Enlargement of the liver and spleen (hepatosplenomegaly), which may distend the abdomen,
- Fever, which is usually intermittent,
- High levels of immune globulin in the blood (hypergammaglobulinemia).
In very advanced disease, the skin may turn dark (hyper-pigmentation), which prompted visceral leishmaniasis (VL) to be called “kala-azar,” which means “black fever”.
The hyper-pigmentation is due to increased melanin in the skin. Inflammatory products due to visceral leishmaniasis (VL) stimulate the pituitary gland to make high levels of adrenocorticotropic hormone, which increases melanin production.
It also affects the kidney, which may lead to renal failure, although some of the anti-leishmanial drugs may also be responsible for kidney toxicity. Leishmaniasis may affect other organs, including the bowel and the lung. 
There are a host of other names for cutaneous or dermal leishmaniasis (CL), including “pian bois” and “chiclero ulcer”. The site of the sand fly bite usually forms a raised papule that expands and ulcerates, with a heaped-up border on the edges. The disease becomes manifest over several weeks. There may be only one lesion, or multiple lesions may appear over time. The skin lesions take on a variety of appearances and may resemble acne, warts, or psoriasis.
They may look like large scaly, ulcerated plaques or form shallow ulcerated nodules. The lesions may be dry or weeping and are not usually painful unless secondarily infected by bacteria. Sores occur predominantly on the extremities and face.
If not treated properly, they heal over months to years, leaving scars that often resemble old burns. In severe cases, such as diffuse cutaneous leishmaniasis, nodular lesions may occur widely and last for years or even for life (if not treated properly).
Mucocutaneous leishmaniasis (ML) involves the nose, mouth, and larynx. It is less common than visceral leishmaniasis (VL) and cutaneous or dermal leishmaniasis (CL).
Initially, the patient experiences a nodule at the site of the sand fly bite with symptoms consistent with cutaneous or dermal leishmaniasis (CL). Subsequently, mucocutaneous involvement leads to nodules inside the nose, perforation of the nasal septum, and enlargement of the nose or lips. If the larynx is involved, the voice changes as well. Ulcerated lesions may lead to scarring and tissue destruction that can be disfiguring.
Diagnosis
In countries where the disease is common, medical professionals may presume that patients with compatible clinical symptoms and findings have leishmaniasis. Other patients require definitive diagnosis, done by examining tissue under a microscope to detect the parasite or through a blood test to detect antibodies.
Full thickness skin biopsy for diagnosis of cutaneous or dermal leishmaniasis (CL), which allows testing for more than one infection.
Bone marrow aspirate is preferred for diagnosis of visceral leishmaniasis (VL) by examining it for amastigotes and sending to a reference laboratory for polymerase chain reaction (PCR) and/or culture.
Lymph nodes, liver, and “buffy coat” (white cells) from a blood specimen may also be used (they may be helpful in immunosuppressed individuals).
Medical professionals can culture the specimen on special media, which allows the parasite to multiply, making detection easier under the microscope.
Anti-leishmanial antibodies in the blood can be detected using enzyme-linked immunosorbent assays (ELISA). Antibody assays are usually positive in visceral leishmaniasis (VL) but are not useful in cutaneous or dermal leishmaniasis (CL) and mucocutaneous leishmaniasis (ML), because these conditions do not stimulate reliably and/or consistently elevated antibody titers in the blood.
Antibody assays may be falsely negative in immunosuppressed individuals with visceral leishmaniasis (VL), and health care providers should use other diagnostic methods.
Allopathic treatment for leishmaniasis 
Because of the diversity of species and manifestations, and lack of extensive data, there is no allopathic drug or treatment for leishmaniasis.
Allopathic medical professionals must individualize treatment based on the species, type of syndrome, and geographic area. Allopathic physicians should consult with CDC experts and an infectious disease specialist.
The few anti-leishmaniasis under experiment drugs are liposomal amphotericin B and oral miltefosine. Amphotericin B has frequent side effects, including renal toxicity. It is the first highly active oral agent for visceral leishmaniasis (VL) Ketoconazole and fluconazole are azole antifungals that may be effective against certain species.
Patients may use traditional agents based on antimony, called pentavalent antimonial (SbV) compounds, intravenously or intramuscularly.
Cutaneous or dermal leishmaniasis (CL) in a person with normal immunity may not require any treatment, depending on severity of the lesion, since it will resolve on its own in several weeks. Health care providers sometimes simply monitor cases with few lesions that are small and appear to be healing. More significant cases of disease is treated with medications, but treatment recommendations vary with where the disease was acquired and the species of Leishmania (if known).
Possible treatments for cases arriving include oral ketoconazole or topical compound of 15% paromomycin. Other treatments include local heat therapy (requires local anesthesia) or repeated cryotherapy with liquid nitrogen over several weeks.
Mucocutaneous leishmaniasis is less common, and there is no clear consensus on treatment.
Prevent leishmaniasis
There is no vaccine for leishmaniasis in allopathic medicines, but in Homeopathic medicines any medicine for leishmaniasis could be advised (in high) as a Homeopathic Vaccine (for profilaction).
The best way to prevent leishmaniasis is to avoid the bite of the sand fly. Simple insect precautions, including protective clothing (long sleeves, shirts tucked into pants, long pants, and socks) and insect repellents.
Homeopathic treatment for leishmaniasis
There are many proven Homeopathic medicines for leishmaniasis for example:

Antimonium Crudum
Eczema with gastric derangements. Pimples, vesicles, and pustules. Thick, hard, honey-colored scabs. Urticaria; measle-like eruption. Itching when warm in bed. Dry skin. Dry gangrene. Scaly, pustular eruption with burning and itching, worse at night. Chilly even in warm room. Intermittent with disgust, nausea, vomiting, eructations, coated tongue, diarrhoea. Hot sweat. Nostrils chapped and covered with crusts. Eczema of nostrils, sore, cracked and scurfy. Pimples, pustules, and boils on face. Yellow crusted eruption on cheeks and chin. Sallow and haggard.
Ledum Palustre
Bites. Stings. Boils. Bruises. Deafness. Ear inflammation. Eczema. Erythema nodosum. Facial pimples. Feet pains; tender. Gout. Haemoptysis. Hands pains. Intoxication. Joints affections, cracking. Meniere’s disease. Pediculosis. Priapism. Prickly heat. Puncture wounds. Rheumatism. Skin eruptions. Stings. Tetanus. Tinnitus. Tuberculosis. Varicella. Whitlow. Wounds.
Anthracinum
This nosode has proven a great medicine in epidemic spleen diseases and in septic inflammation, carbuncles and malignant ulcers. Boils and boil-like eruptions, acne. Terrible burning. Induration of cellular tissue, abscess, bubo, and all inflammation of connective tissue in which there exists a purulent focus.
Tissues haemorrhages, black, thick, tar-like, rapidly decomposing, from any orifice. Glands swollen, cellular tissues oedematous and indurated. Septicaemia. Ulceration, sloughing and intolerable burning. Erysipelas. Black and blue blisters. Dissecting wounds. Insect stings. Bad effects from inhaling foul odors. Gangrenous parotitis. Succession of boils. Gangrene. Foul secretions.
Tarentula Cubensis
Red spots and pimples. Feels puffed all over. Carbuncles, burning, stinging pains. Purplish hue. Gangrene. Abscesses, where pain and inflammation predominate. Scirrhous of breasts. “Senile” ulcers. A toxaemic medicine, septic conditions. Diphtheria. Adapted to the most severe types of inflammation and pain, early and persistent prostration. Various forms of malignant suppuration. Purplish hue and burning, stinging pains. Bubo. Pain of death – Sever pain; soothes the last struggles. Pruritus, especially about genitals. Restless feet. Intermittent septic chills. Bubonic plague. As a curative and preventive remedy especially during the period of invasion. Stomach feels hard, sore.
Pyrogenium
Pyrogen is the medicine of choice for septic states, with intense restlessness. “In septic fevers, especially puerperal. Hectic, typhoid, typhus, ptomaine poisoning, diphtheria, dissecting wounds, sewer-gas poisoning, chronic malaria, after-effects of miscarriage, all discharges are horribly offensive-menstrual, lochial, diarrhoea, vomit, sweat, breath, etc. Great pain and violent burning in abscesses. Chronic complaints that date back to septic conditions. Threatening heart failure in zymotic and septic fevers. Influenza, typhoid symptoms. Small cut or injury becomes much swollen and inflamed-discolored. Tongue red and dry, clean, cracked, smooth, as though varnished. Throat dry, articulation difficult. Nausea and vomiting. Taste terribly fetid. Breath horrible.
Coffee-grounds vomiting. Vomits water, when it becomes warm in stomach. Intolerable tenesmus o both bladder and rectum. Bloated, sore, cutting pain. Diarrhoea; horribly offensive, brown-black, painless, involuntary. Constipation, with complete inertia; obstinate from impaction. Stools large, black, carrion-like, or small black balls.
Lachesis Mutus
Like all snake poisons, Lachesis decomposes the blood, rendering it more fluid; hemorrhagic tendency is marked. Purpura, septic states, diphtheria, and other forms of disease, when the system is thoroughly poisoned and the prostration is profound.
The modalities are most important in guiding to the medicine. Delirium tremens with much trembling and confusion. Very important during the climacteric and for patients of a melancholic disposition. Ill effects of suppressed discharges. Diphtheritic paralysis. Diphtheria carriers. Sensation of tension in various parts. Hepatomegaly, painful. Abdomen tympanitic, sensitive, painful. Hot perspiration, bluish, purplish appearance. Boils, carbuncles, ulcers, with bluish, purple surroundings. Dark blisters. Bed-sores, with black edges. Blue-black swellings. Pyemia; dissecting wounds. Purpura, with intense prostration. Senile erysipelas. Wens. Cellulitis. Varicose ulcers.
Crotalus Horridus
Itching stinging all over; urticaria. Skin dry, stiff like thin parchment; usually cold. Yellow colour of
whole body (haematic rather than hepatic jaundice). Petechiae. Vesicles; herpes; pimples; boils; carbuncles; burns; stings; pemphigus; ulcers; gangrene; felons; anthrax. Bilious fever. Boils. Cancers. Carbuncles. Cerebro-spinal meningitis. Chancre. Ciliary neuralgia. Convulsions. Delirium tremens. Dementia. Diphtheria. Dysmenorrhoea. Dyspepsia. Otitis. Ecchymosis. Epilepsy. Eyes affections. Erysipelas. Face eruption; distortion. Haematuria. Haemorrhagic diathesis. Headache. Heart affections. Hydrophobia. Intestinal haemorrhage. Jaundice. Keratitis. Liver disorders. Lungs affections. Mastitis. Measles. Milk-leg. Meningitis. Ovaries affections. Ozaena. Palpitation. Peritonitis. Perityphlitis. Phlebitis. Psoriasis palmaris. Purpura. Pyaemia. Remittent fever. Smallpox. Stings. Syphilis. Tetanus. Thirst. Tongue inflammation; tongue cancer. Ulcers. Urticaria. Vaccination effects. Varicosis. Varicocele. Vomiting, bilious.
Hippozinum
Consumption, cancer, syphilis, etc, and promises useful service in the treatment of ozaena, scrofulous swellings, pyaemia, erysipelas. Chronic rhinitis; saneous secretion. Nose red, swollen. Catarrh, ozaena, ulceration. Discharge acrid, corroding, bloody, offensive. Tubercles on alae nasi. Papules and ulceration in frontal sinus and pharynx. All glands swollen; painful; form abscesses. Hoarseness. Bronchial asthma. Noisy breathing; short, irregular. Cough, with dyspepsia. Excessive secretion. Suffocation imminent. Bronchitis in the aged, where suffocation from excessive secretion is imminent. Tuberculosis. Lymphatic swellings. Articular non-fluctuating swellings. Nodules in arm. Malignant erysipelas. Pustules and abscesses. Ulcers. Rupia. Eczema.
Echinacea Angustifolia
Recurring boils. Carbuncles. Irritations from insect bites and poisonous plants. Lymphatics enlarged. Old tibial ulcers. Gangrene. Remarkable medicine as a “corrector of blood dyscrasia”. Acute auto-infection. Blood poisoning, septic conditions. Diarrhoea in typhoid. Gonorrhoea. Boils. Erysipelas and foul ulcers. Gangrene. Goitre with exophthalmic symptoms. Tendency to malignancy in acute and subacute disorders. Last stages of cancer to ease pain. Venom infection. Cerebro-spinal meningitis. Puerperal infections. Tired feeling. Piles. Pustules.
Acts on vermiform appendix thus has been used for appendicitis, but remember it promotes suppuration and a neglected appendicitis with pus formation would probably rupture sooner under its use. Lymphatic inflammation; crushing injuries. Snake bites and bites and stings generally. Foul discharges with emaciation and great debility.
Antim Crudum
Eczema with gastric derangements. Pimples, vesicles, and pustules. Thick, hard, honey-colored scabs. Urticaria; measle-like eruption. Itching when warm in bed. Dry skin. Warts. Dry gangrene. Scaly, pustular eruption with burning and itching, worse at night.
Silica Tera 
Felons, abscesses, boils, old fistulous ulcers. Delicate, pale, waxy. Cracks at end of fingers. Painless swelling of glands. Rose-colored blotches. Scars suddenly become painful. Pus offensive. Promotes expulsion of foreign bodies from tissues. Every little injury suppurates. Long lasting suppuration and fistulous tracts. Dry fingertips. Eruptions itch only in daytime and evening. Crippled nails. Indurated tumors. Abscesses of joints. After impure vaccination. Bursa. Lepra, nodes, and coppery spots. Keloid growths.
Chilliness; very sensitive to cold air. Creeping, shivering over the whole body. Cold extremities, even in a warm room. Sweat at night; worse towards morning. Suffering parts feel cold.
Asafetida
Itching, better by scratching; pricking, burning skin. Ulcers with high, hard edges, sensitive to touch, easily bleeding; old ulcers on forearm, wrist, hand; ulcers, esp. when affecting the bones; pus profuse, greenish, thin, offensive, even ichorous. Ulcers, very painful to contact, esp. in the circumference, gangrenous.
Leishmania Nosode
Nosodes are specialized Homeopathic remedies that are prepared by taking actual diseased matter such as diseased tissue or nasal discharge from a sick/infected person. The preparation of a nosode involves a lengthy process of succussion and dilution of the original material using traditional homeopathic protocols until virtually no molecules of the crude substance remain, rendering the nosode safe for use.
Inactivates the original disease substance and converts the material into a bioenergetic remedy, which interacts with the body’s energy field. The final product is a potent remedy that is an energetic blueprint of the actual disease and can actually stimulate dogs immune system to ward off the disease.
Use of nosode in outbreak of disease gives results with the great success. It is my (Dr Qaisar Ahmed) professional opinion based on years of clinical experience with homeopathic medicines that any nosode in combination can provide significant and safe protection which is also inexpensive in comparison with the conventional vaccine.
My (Dr Qaisar Ahmed) clinical studies measure the rate of protection provided by any nosodes is higher than any other allopathic vaccine.
China Officinalis
Extreme sensitiveness to touch, but hard pressure relieves. Coldness; much sweat. One hand ice cold, the other warm. Anasarca. Dermatitis; erysipelas. Indurated glands; scrofulous ulcers and caries. Intermittent, paroxysms anticipate; return every week. All stages well marked. Chill generally in forenoon, commencing in breast; thirst before chill, and little and often. Debilitating night-sweats. Free perspiration caused by every little exertion, especially on single parts. Hay fever, watery coryza, pain in temples.
Arsenicum Album
Itching, burning, swellings; oedema, eruption, papular, dry, rough, scaly; worse cold and scratching. Malignant pustules. Ulcers with offensive discharge. Anthrax. Poisoned wounds. Urticaria, with burning and restlessness. Psoriasis. Scirrhus. Icy coldness of body. Epithelioma of the skin. Gangrenous inflammations. High temperature. Periodicity marked with adynamia. Septic fevers. Intermittent. Paroxysms incomplete, with marked exhaustion. Hay-fever. Cold sweats. Typhoid. Complete exhaustion. Delirium; worse after midnight. Great restlessness
Aranea Diadema
Bones affections. Catalepsy. Chills. Dysmenorrhoea. Dyspepsia. Haemorrhages. Haemorrhagic diathesis. Headache. Hydrogenoid constitution. Intermittents. Malarial cachexia. Menstruation irregularities. Neuralgia. Puncture wounds. Scorbutic affections. Scurvy rickets. Spleen affections.
P. S: This article is only for doctors having good knowledge about Homeopathy and allopathy, for learning purpose(s).
For proper consultation and treatment, please visit our clinic.
None of above-mentioned medicine(s) is/are the full/complete treatment but just hints for treatment; every patient has his/her own constitutional medicine.
 Dr Qaisar Ahmed – Gastroenterologist, Specialist Homeopathic Medicines.
Dr Qaisar Ahmed – Gastroenterologist, Specialist Homeopathic Medicines.
Senior research officer at Dnepropetrovsk state medical academy Ukraine.
Location: Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Find more about Dr Sayed Qaisar Ahmed at:
https://www.youtube.com/Dr Qaisar Ahmed
https://www.facebook.com/ahmed drqaisar
Glad to be one of the visitants on this awing website : D.