
Diphtheria manifests as either an upper respiratory tract or cutaneous infection and is caused by the aerobic gram-positive bacteria, Corynebacterium diphtheria.
People who are most susceptible to infection are those who are not completely immunized/low antitoxin antibody levels and have been exposed to a carrier or diseased individual.
A carrier is someone whose cultures are positive for the diphtheria species but does not exhibit signs and symptoms. As the number of asymptomatic carriers decrease, the number of diphtheria cases consequently decline.
Corynebacterium diphtheria is a nonencapsulated, nonmotile, gram-positive bacillus. Pathogenic strains can result in severe localized upper respiratory infection, localized cutaneous infections, and rarely systemic infection. Exotoxins are associated with both invasive localized and systemic forms of this disease.
Exotoxins are encoded in viral bacteriophages, which are transmitted from bacteria to bacteria. The 3 isolated strains of C diphtheria include gravis, intermedius, and mitis. Intermedius is thought to be responsible for systemic elaboration of the disease, as it is most often associated with the exotoxin. However, all 3 strains can produce toxins.
C diphtheria adheres to mucosal epithelial cells where the exotoxin, released by endosomes, causes a localized inflammatory reaction followed by tissue destruction and necrosis.
Cutaneous diphtheria is characterized by indolent, nonhealing ulcers covered with a gray membrane. The ulcers often are co-infected with Staphylococcus aureus and group A streptococci. This form of the disease is seen with increasing frequency in poor, inner-city dwellers and alcoholics.
The lesions of cutaneous diphtheria are infectious, and bacteria from cutaneous lesions have been found to cause pharyngeal infections and thus serve as a reservoir for infection.
Corynebacterium ulcerans is a relatively rare species that more frequently causes cutaneous diphtheria; however, this species may rarely cause respiratory symptoms. Disease severity is dependent on exotoxin production.
C ulcerans also has been linked to zoonotic transmission to humans and most frequently has been seen in agricultural communities associated with livestock.
Human carriers are the main reservoir of infection; however, case reports have linked diphtheria to livestock. Infected patients and asymptomatic carriers can transmit C diphtheria via respiratory droplets, nasopharyngeal secretions, and rarely fomites. In cutaneous disease, contact with wound exudates may result in the transmission of the disease to the skin as well the respiratory tract.
Symptoms and incubation
Diphtheria symptoms typically follow an incubation period of 2-5 days (range, 1-10 d). Symptoms initially are general and nonspecific, often resembling a typical viral upper respiratory infection (URI). Respiratory involvement usually begins with sore throat and mild pharyngeal inflammation. Development of a localized or coalescing pseudomembrane can occur in any portion of the respiratory tract. The pseudomembrane is characterized by the formation of a dense, gray debris layer composed of a mixture of dead cells, fibrin, RBCs, WBCs, and organisms. Removal of the membrane reveals a bleeding, edematous mucosa.
A combination of cervical adenopathy and swollen mucosa imparts a “bull’s neck” appearance. The most frequent cause of death is the quick progress of respiratory diphtheria to respiratory failure which causes the airway obstruction or aspiration of pseudo membrane into the tracheobronchial tree.
Complains
Patients with diphtheria may present with the following complaints:
-
Low-grade fever (rarely >103°F) (50-85%) and chills,
-
Malaise, weakness, prostration,
-
Sore throat (85-90%),
- Hoarseness, dysphagia (26-40%),
-
Headache,
-
Cervical lymphadenopathy and respiratory tract pseudomembrane formation (about 50%),
-
Serosanguineous or seropurulent nasal discharge, white nasal membrane,
-
Dyspnea, respiratory stridor, wheezing, cough.
Cutaneous diphtheria often develops at a site of previous trauma or a primary dermatologic disease. It follows an indolent course, typically lasting weeks to months. Occasionally, it may cause respiratory diphtheria.
Patient has a low-grade fever but is toxic in appearance and also may have a swollen neck.
Pharyngeal diphtheria: 
-
Patients may present with general symptoms of fever, halitosis, tachycardia, and anxiety.
-
Tonsils and pharynx: Pharyngeal erythema and edema; thick, gray, leathery membrane variably covers the tonsils, soft palate, oropharynx, nasopharynx, and uvula. Attempts at scraping the pseudomembrane cause bleeding of the underlying mucosa.
-
Neck: Extensive anterior and submandibular cervical lymphadenopathy imparts a bull’s neck appearance. The patient may hold his or her head in extension. It occasionally can also be associated with dysphonia.
-
Respiratory distress manifesting as stridor, wheezing, cyanosis, accessory muscle use, and retractions.
Cardiac toxicity typically occurs after 1-2 weeks of illness following improvement in the pharyngeal phase of the disease. It may manifest as follows:
-
Myocarditis is seen in as many as 60% of patients (especially if previously unimmunized) and can present acutely with congestive heart failure (CHF), circulatory collapse, or more subtly with progressive dyspnea, diminished heart sounds, cardiac chamber dilatation, and weakness.
-
Atrioventricular blocks, ST-T wave changes, and various dysrhythmias may be evident.
-
Endocarditis may be present, especially in the presence of an artificial valve.
Neurologic toxicity is proportional to the severity of the pharyngeal infection. Most patients with severe disease develop neuropathy. Deficits include the following:
Differential Diagnoses 
- Angioedema
- Emergent Management of Pediatric Epiglottitis
- Epiglottitis
- Infective Endocarditis
- Infectious Mononucleosis (IM)
- Myocarditis
- Oropharyngeal/esophageal candidiasis
- Pharyngitis
- Peritonsillar Abscess
- Retropharyngeal Abscess
- Rheumatic Fever
- Septic Shock.
Diagnosis/Laboratory Studies
To establish the diagnosis of C diphtheriae, it is vital to both isolate C diphtheriae in culture media and to identify the presence of toxin production.
Bacteriologic testing
Gram stain shows club-shaped, nonencapsulated, nonmotile bacilli found in clusters.
Immunofluorescent staining of 4-hour cultures or methylene blue–stained specimen may sometimes allow for a speedy identification.
Toxigenicity
Toxigenicity testing is aimed at determining the presence of toxin production.
Other laboratory studies
- CBC may show moderate leukocytosis.
- Urinalysis (UA) may demonstrate transient proteinuria.
- Serum antibodies to diphtheria toxin prior to administration of antitoxin: Low levels cannot exclude the possibility of the disease; high levels may protect against severe illness (concentrations of 0.1 to 0.01 IU are thought to confer protection).
- Serum troponin I levels seem to correlate with the severity of myocarditis.
- Chest radiograph and soft tissue neck radiography/CT or ultrasonography may show prevertebral soft tissue swelling, enlarged epiglottis, and narrowing of the subglottic region.
- Echocardiography may demonstrate valvular vegetations; however, this systemic manifestation of diphtheria is rare. ECG may show ST-T wave changes, variable heart block, and dysrhythmia.
Procedures
The following procedures may be necessary:
-
Endotracheal intubation,
-
Surgical airway – Cricothyrotomy or tracheostomy,
-
Laryngoscopy, bronchoscopy as indicated in intubated patients,
-
Electrical pacing for high-grade conduction disturbances.
Emergency Department Care 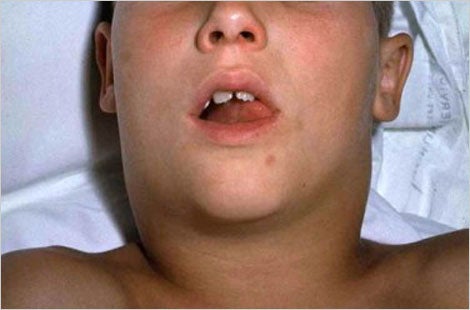
Treatment of diphtheria should be initiated even before confirmatory tests are completed due to the high potential for mortality and morbidity. Isolate all cases promptly. Early airway management allows access for mechanical removal of tracheobronchial membranes and prevents the risk for sudden asphyxia through aspiration. An ENT personnel should take care for intubation and securing of airway if there is suspicion for loss of the airway or respiratory failure. Maintain close monitoring of cardiac activity for early detection of rhythm abnormalities.
Initiate prompt antibiotic coverage (allopathic – erythromycin or penicillin; Homeopathic -Diphtherinum, Merc Sole/Merc Iod or Hepar Sulph or Tuberculinum, any one along with Belladonna) for eradication of organisms, thus limiting the amount of toxin production. Antibiotics hasten recovery and prevent the spread of the disease to other individuals.
Neutralize the toxin as soon as diphtheria is suspected. Diphtheria antitoxin is a horse-derived hyperimmune antiserum that neutralizes circulating toxin prior to its entry into the cells. It prevents the progression of symptoms. The dose and route of administration of allopathic medicines (IV vs IM) are dependent on the severity of the disease.
The patient must be tested for sensitivity to allopathic antitoxin before it is given.
Allopathic Medication/Treatment
Patients with active disease as well as all close contacts should be treated with antibiotics, which is most effective in the early stages of disease and decreases the transmissibility and improves the course of diphtheria.
Close contacts, such as family members, household contacts, and potential carriers, must receive chemoprophylaxis regardless of immunization status or age. This entails treatment with erythromycin or penicillin for 14 days and post treatment cultures to confirm eradication.
Macrolides such as erythromycin as first-line agents for patients older than 6 months of age. However, macrolide therapy has been associated with an increase in pyloric stenosis in children younger than 6 months, especially treatment with erythromycin. Intramuscular penicillin is recommended for patients who will be noncompliant or intolerant to an erythromycin course.
The horse serum antitoxin is given to anyone suspected to have diphtheria and can be administered without confirmation from cultures, as it is most efficacious early during the course of the disease.
Diphtheria disease does not confer immunity; thus, initiation or completion of immunization with diphtheria toxoid is necessary.
Obtain throat and nasal swabs from persons in close contact with the suspected diphtheria victim; administer age-appropriate diphtheria booster. Throat cultures should be repeated in 2 weeks after treatment. 00225-X/asset/adc370f5-df5f-4d70-bf26-521070396ba2/main.assets/gr1_lrg.jpg)
Antitoxins
Diphtheria antitoxin (derived from a horse serum), neutralizes unbound exotoxin. It is to be administered as soon as diphtheria suspected. Administer immunization toxoid booster, as the antitoxin does not influence immunity.
Diphtheria antitoxin
Neutralizes toxin before it enters cells. Dose given depends on site of infection and length of time patient is symptomatic.
Macrolides
Erythromycin and penicillin are both recommended for the treatment of diphtheria. Penicillin is recommended in household contacts who may not comply with the duration of erythromycin treatment, however, resistant strains and transmission from penicillin-treated carriers has been reported. An increased incidence of pyloric stenosis is associated with administration of erythromycin to infants younger than 6 months. It is believed that azithromycin may be a better macrolide treatment in this population, though there are a few case reports describing pyloric stenosis in infants treated with azithromycin for pertussis infections.
The treatment of endocarditis requires the addition of an aminoglycoside.
Erythromycin
Age, weight, and severity of infection determine proper dosage in children. When bid dosing is desired, one half the total daily dose may be taken q12h. Double the dose for more severe infections.
Erythromycin has the advantage of being a good anti-inflammatory agent by inhibiting migration of polymorphonuclear leukocytes.
Penicillin G benzathine
Interferes with synthesis of cell wall mucopeptides during active multiplication, which results in bactericidal activity. Effective treatment for systemic diphtheria.
Vaccination
The use of diphtheria and tetanus toxoids and acellular pertussis vaccine (DTaP) has greatly decreased the incidence of diphtheria. Although childhood DTaP coverage exceeds 80%, acquired immunity wanes over time, requiring a booster to preserve immunity.
Although vaccination is not guaranteed to prevent diphtheria, vaccinated persons who later develop diphtheria have been reported as having milder and fewer fatal infections.
Homeopathic “Diphtherinum, Variolinum or Merc Iodum” in high doses gives best long lasting immunity against diphtheria.
The most widely quoted diphtheria mortality rate is 5-10%. It may reach higher than 20% in children younger than 5 years and adults older than 40 years. Immunization patterns have the most influence on mortality patterns.
Mortality rates have not changed significantly over the past few decades. Most deaths occur on days 3-4 secondary to asphyxia with a pharyngeal membrane or due to myocarditis. Mortality rates of 30-40% have been reported for bacteremic disease.
Homeopathic Management/Treatment for diphtheria
Here are few examples of these Homeopathic medicines: 
Diphtherinum
A nosode, trituration of diphtheritic membrane. Dilutions of diphtheria toxin.
The well-known features of the disease of which this nosode is a product must be the guide to its use. It is more afficative in high potencies against diphtheria, both as prophylactic and cure, than the allopathic serum injections. It is very useful in the paralysis of diphtheria and other like kinds of spinal affection. Croup. Diphtheria. Diphtheritic paralysis. Myelitis.
Mercurius Dulcis
Has marked effect on catarrhal inflammation of ear, and useful in Eustachian catarrh, deafness. Diarrhoea. Prostatitis. Remittent bilious attacks. Pallor, flabby bloatedness, and turgid flaccidity. Diphtheria. Inflammation with plastic exudate. Peritonitis and meningitis with plastic exudate. Dropsies due to combined renal and cardiac diseases, especially with jaundice. Cirrhosis of the liver, especially in the hypertrophic form. Otitis media; closure of Eustachian tube; ear troubles of scrofulous children; membrana tympani retracted, thickened and immovable.
Offensive breath; salivation; sore gums. Ulcers. Tongue black. Constant flow of dark, putrid saliva; very offensive. Ulceration of throat, with dysphagia. Granular pharyngitis.
Merc Iodum
Throat affections, with greatly swollen glands and characteristic coating of tongue. Diphtheria. Chancre; induration remains long time. Swollen inguinal glands, large and hard. Mammary tumors. Tongue coated thickly; yellow at the base. Tip and edges may be red and take imprint of teeth.
Lacunar tonsillitis. Cheesy exudates with offensive breath. Ulcers on posterior pharynx. Easily detached patches on inflamed pharynx and fauces; much tenacious mucus. Sensation of a lump. Constant inclination to swallow.
Mercurius Cyanatus
Acute infections, pneumonia, nephritis. Septicemia. Diphtheria, malignant types, with prostration. Coldness and nausea. Syphilitic ulcers when perforation threatens. Great and rapid prostration, tendency toward haemorrhages, from the different orifices, of dark fluid blood, cyanosis, rapid respiration and heart action, albuminuria and twitching and jerking of muscles. Typhoid pneumonia. Livid states from great struggling. Suffocation.
Mouth covered with ulcerations. Tongue pale. Free salivation. Fetor of breath. Pain and swelling of salivary glands. Astringent taste. Ulcerations of mouth have a gray membrane.
Throat feels raw and sore. Mucous membranes broken down, ulcerated. Looks raw in spots. Hoarseness, and talking is painful. Necrotic destruction of soft parts of palate and fauces. Intense redness of fauces. Swallowing very difficult. Dark blood from nose. Diphtheria of the larynx and nose.
Kalium Muriaticum
Aphthae; thrush; white ulcers in mouth. Swollen glands about jaw and neck. Coating of tongue grayish-white, dryish, or slimy. Follicular tonsillitis. Tonsils inflamed; enlarged so much, can hardly breathe. Grayish patches or spots in the throat and tonsils. Adherent crusts in vault of pharynx. “Hospital” sore throat. Eustachian catarrh. Diphtheria. Loss of voice; hoarseness. Asthma, with gastric derangements; mucus white and hard to cough up. Loud, noisy stomach cough; cough short, acute, and spasmodic, like whooping-cough; expectoration thick and white. Rattling sounds of air passing through thick, tenacious mucus in the bronchi; difficult to cough up.
Chronic, catarrhal conditions of the middle ear. Glands around the ear swollen. Snapping and noises in the ear. Threatened mastoid. Great effusion about the auricle. Cheek swollen and painful.
Tuberculinum 
Enlarged tonsils. Hard, dry cough during sleep. Expectoration thick, easy; profuse bronchorrhea. Shortness of breath. Sensation of suffocation. Diphtheria. Bronchopneumonia. Hard, hacking cough, profuse sweating and loss of weight, rales all over chest. Deposits begin in apex of lung.
Aconitum Napellus
A best anti inflammatory medicine. Acute, sudden, and violent invasion. Does not want to be touched. Sudden and great sinking of strength. Complaints and tension caused by cold weather, draught of cold air, checked perspiration. Serous membranes and muscular tissues affected markedly. Burning in internal parts; tingling, coldness and numbness. Influenza. Diphtheria. Tension of arteries. Influenza.
Its sphere is in the beginning of an acute disease and not to be continued after pathological change comes. In Hyperaemia, congestion not after exudation has set in.
Apis Mellifica
Tongue fiery red, swollen, sore, and raw, with vesicles. Scalding in mouth and throat. Diphtheria. Membrane of mouth and throat glossy, red, shining, and puffy, like erysipelas. Cancer of the tongue. Throat constricted, stinging pains. Uvula swollen, sac-like. Throat swollen, inside and out; tonsils swollen, puffy, fiery red. Ulcers on tonsils. Fiery red margin around leathery membrane. Hoarseness; dyspnoea, breathing hurried and difficult. Edema of larynx. Suffocation; short, dry cough, suprasternal. Hydrothorax.
Bromium
Throat feels raw, hoarseness. Tonsils pain on swallowing, deep red, with network of dilated blood vessels. Tickling in trachea during inspiration. Whooping cough. Dry cough, with hoarseness and burning pain behind sternum. Spasmodic cough, with rattling of mucus in the larynx; suffocative. Hoarseness. Croup after febrile symptoms have subsided. Difficult and painful breathing. Diphtheria. Laryngeal diphtheria, membrane begins in larynx and spreads upward. Spasmodic constriction. Asthma; difficulty in getting air into lung. Hypertrophy of heart. Fibrinous bronchitis, great dyspnoea. Bronchial tubes feel filled with smoke.
Baptisia Tinct
Dark redness of tonsils and soft palate. Constriction, contraction of oesophagus. Great difficulty in swallowing solid food. Painless sore throat, and offensive discharge. Diphtheria. Contraction at cardiac orifice. Lungs feel compressed, breathing difficult; seeks open window. Fears going to sleep on account of nightmare and sense of suffocation. Constriction of chest. Septic conditions.
Cardus Marianus
Tongue white in centre; red tip and edges; white-coated on side. Collection of water in mouth. Smooth sensation of mucous membrane of palate as though covered with fat. Diphtheria. Irritation in posterior part of larynx causing cough. Expectoration: pure blood; mucus mixed with blood. Pain pressure and stitches in region of heart; oppression on deep breathing.
Cantharis Vesicatoria
Tongue covered with vesicles; deeply furred; edges red. Burning in mouth, pharynx, and throat; vesicles in mouth. Great difficulty in swallowing. Very tenacious mucus. Violent spasms reproduced by touching larynx. Inflammation of throat; feels on fire. Constriction; aphthous ulceration. Scalding feeling. Diphtheria.
Acidum Nitricum
Pain into ears. Hawks mucus constantly. White patches and sharp points, as from splinters, on swallowing. Diphtheria. Nasal diphtheria, with watery and exceedingly excoriating discharge. Hoarseness. Aphonia, with dry hacking cough.
Kalium Brichromicum 
The special effects of this medicine are the mucous membrane of stomach, bowels, air-passages; bones, fibrous tissues, kidneys, heart, and the liver. Perforation of the septum. Throat fauces red and inflamed., dry and rough. Parotid glands swollen. Uvula relaxed, oedematous. Pseudomembranous deposit on tonsils and soft palate. Diphtheria, with profound prostration and soft pulse. Discharge from mouth and throat, tough and stringy. Mouth dry; viscid saliva. Tongue mapped, red, shining, smooth, and dry, with dysentery; broad, flat, indented, thickly coated.
Voice hoarse. Metallic, hacking cough. Profuse, yellow expectoration, very glutinous and sticky, coming out in long, stringy, and very tenacious. Tickling in larynx. Catarrhal laryngitis cough has a brassy sound. True membranous croup, extending to larynx and nares. Cough, with pain in sternum, extending to shoulders. Pain at bifurcation of trachea on coughing; from mid-sternum to back.
Heart – dilatation, especially from coexisting kidney lesion. Cold feeling around heart.
Allium Capa
Hoarseness. Hacking cough on inspiring cold air. Tickling in larynx. Sensation as if larynx is split or torn. Oppressed breathing from pressure in middle of chest. Diphtheria. Constricted feeling in region of epiglottis. Pain extending to ear. Copious, watery and extremely acrid discharge. Feeling of a lump at root of nose.
Arsenicum Album
Throat – swollen, oedematous, constricted, burning, unable to swallow. Diphtheritic membrane dry and wrinkled, ulcerated with blue color. Bloody saliva. Suffocation -air-passages constricted. Expectoration scanty, frothy. Wheezing respiration. Haemoptysis. Palpitation, pain, dyspnoea, faintness. Irritable heart. Pulse more rapid in morning. Dilatation. Cyanosis. Fatty degeneration. Diphtheria.
Suffocation. Air passages constricted. Burning in chest. Suffocative catarrh. Expectoration scanty, frothy. Wheezing respiration. Haemoptysis with pain between shoulders; burning heat all over.
Heart – Palpitation, pain, dyspnoea, faintness. Irritable heart. Pulse more rapid in morning. Dilatation. Cyanosis. Fatty degeneration. Angina pectoris, with pain in neck and occiput.
Medorrhinum
Chronic catarrhal conditions. Chronic nasal and pharyngeal catarrhs. Tongue coated brown and thick, blistered; canker sores. Blisters on inner surface of lips and cheeks. Oppression of breathing. Hoarse while talking. Pain and soreness through chest and mammae. Incessant, dry, night cough. Asthma. Incipient consumption. Larynx feels sore. Diphtheria. Dyspnoea; cannot exhale. Cough; better lying on stomach.
Sambucus Nigra
Acts especially on the respiratory organs. Dry coryza. Diphtheria. Chest oppressed with pressure in stomach, and nausea Hoarseness with tenacious mucus in larynx. Paroxysmal, suffocative cough, coming on about midnight, with crying and dyspnoea. Spasmodic croup. Sniffles of infants; nose dry and obstructed. Loose choking cough. Hands turn blue. Edematous in legs, insteps, and feet.
Mephitis Putorius 
Best choice for whooping-cough, diphtheria etc. it should be given in the lower dilutions from 1x to 3x. Suffocative feeling, asthmatic paroxysms, spasmodic cough; patient must be raised up, gets cyanotic, cannot exhale, Mucous rales through upper part of chest. Bloated face. Coppery taste, as after eating onions.
Sudden contraction of glottis, when drinking or talking. Food goes down wrong way. False croup; cannot exhale. Few paroxysms in day-time, but many at night; with vomiting after eating. Awakes at night with rush of blood to lower legs.
Drosera Rotundifolia
Spasmodic, dry irritative cough, like whooping-cough, the paroxysms following each other very rapidly; can scarcely breathe; chokes. Diphtheria; yellow expectoration, with bleeding; retching. Deep, hoarse voice; hoarseness; laryngitis. Rough, scraping sensation deep in the fauces and soft palate. Sensation as if crumbs were in the throat, of feather in larynx. Laryngeal phthisis, with rapid emaciation. Asthma when talking, with contraction of the throat at every word uttered.
Corallium Rubrum
Develop much coryza and epistaxis, ulceration within the nostrils. Whooping and spasmodic coughs, especially when the attack comes on with a very rapid cough, and the attacks follow so closely as to almost run into each other. Diphtheria. Patient becomes purple in face. Violence of paroxysm, with expectoration of blood. Painful ulcer in nostrils. Post-nasal catarrh. Profuse secretion of mucus dropping through posterior nares; air feels cold. Epistaxis.
Hawking of profuse mucus. Throat very sensitive, especially to air. Dry, spasmodic, suffocative cough; very rapid, short, barking, with great sensitiveness of air-passages.
Aurum Metallicum
Glands swollen in scrofulous subjects. Palpitation and congestions. Ascites with heart affections. Nose ulcerated, painful, swollen, obstructed, inflamed; caries; fetid discharge, purulent, bloody. Throat stitches when swallowing; pain in glands. Caries of the palate. Diphtheria. Sensation as if the heart stopped beating for two or three seconds, immediately followed by a tumultuous rebound, with sinking at the epigastrium. Palpitation. Pulse rapid, feeble, irregular. Hypertrophy. High Blood Pressure-Valvular lesions of arterio-sclerotic nature.
Hepar Sulphuricum
Loses voice and coughs when exposed to dry, cold wind. Hoarseness, with loss of voice. Cough troublesome when walking. Dry, hoarse cough. Cough excited whenever any part of the body gets cold or uncovered, or from eating anything cold. Croup with loose, rattling cough; worse in morning. Choking cough. Rattling, croaking cough; suffocative attacks; has to rise up and bend head backwards. Anxious, wheezing, moist breathing, asthma worse in dry cold air; better in damp. Palpitation of heart. Diphtheria. Scrofulous and lymphatic constitutions. Ptyalism. Gums and mouth painful to touch and bleed readily.
Sensation as if a plug and of a splinter in throat. Quinsy, with impending suppuration. Stitches in throat extending to the ear when swallowing. Hawking up of mucus.
Myristica Sebifera
A great antiseptic and anti inflammation of skin, cellular tissue and periosteum. Traumatic infections. Parotitis. Fistulas. Carbuncles. Specific action in panaritium. Diphtheria. Coppery taste and burning in throat. Tongue white and cracked. Phlegmonous inflammations. Hastens suppuration and shortens its duration. Inflammation of middle ear, suppurative stage. Fistula in ano. Acts more powerfully often than Hepar sulph and silica.
Calcarea Sulphurica 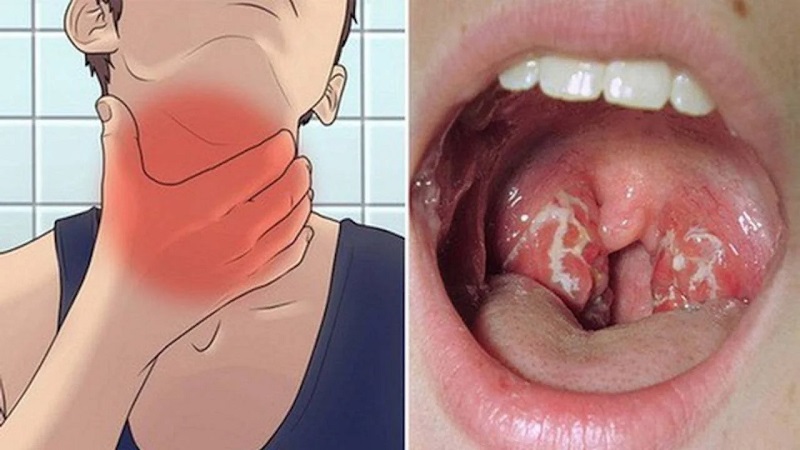
Last stage of ulcerated sore throat, with discharge of yellow matter, yellowish, purulent secretion, frequently tinged with blood. One-sided discharge from nose. Yellowish discharge from posterior nares. Suppurating stage of tonsillitis, when abscess is discharging. Diphtheria. Eczema and torpid glandular swellings. Cystic tumors. Fibroids. Cough, with purulent and sinuous sputa and hectic fever. Empyema, pus forming in the lungs or pleural cavities. Purulent, sanious expectoration. Catarrh, with thick, lumpy, white-yellow or pus-like secretion.
Lycopodium Clavatum
Diphtheria. Diphtherial deposits spread from right to left; worse, cold drinks. Ulceration of vocal bands. Dryness of throat, without thirst. Food and drink regurgitates through nose. Inflammation of throat, with stitches on swallowing. Swelling and suppuration of tonsils. Ulceration of tonsils. Diphtherial deposits spread from right to left; worse, cold drinks. Ulceration of vocal bands. Tubercular laryngitis, especially when ulceration commences.
Tickling cough. Dyspnoea. Tensive, constrictive, burning pain in chest. Cough deep, hollow. Expectorations gray, thick, bloody, purulent, salty. Neglected pneumonia. Aneurysm. Aortic disease. Palpitation at night. Inflammation of throat, with stitches on swallowing. Tubercular laryngitis.
Phosphorus
Irritation, inflammation and degeneration of mucous membranes, serous membranes, spinal cord and nerves, causing paralysis. Destroyed bones. Septicemia. Jaundice. Yellow atrophy of the liver and sub-acute hepatitis.
Larynx very painful. Diphtheria. Clergyman’s sore throat; violent tickling in larynx. Aphonia, with rawness. Sweetish taste while coughing. Hard, dry, tight, racking cough. Congestion of lungs. Burning pains, heat and oppression of chest. Tightness across chest; great weight on chest. Sharp stitches in chest; respiration quickened, oppressed. Heat in chest. Pneumonia, with oppression. Whole body trembles, with cough. Sputa rusty, blood-colored, or purulent. Tuberculosis. Repeated haemoptysis. Pain in throat on coughing. Nervous coughs provoked by strong odors, entrance of a stranger; worse in the presence of strangers; worse lying on left side; in cold room.
Violent palpitation with anxiety. Pulse rapid, small, and soft. Heart dilated, especially right. Feeling of warmth in heart.
Lachesis
Purpura, septic states, diphtheria, and other low forms of disease, when the septicemia and prostration is present. Diphtheritic paralysis. Diphtheria carriers. Sensation of tension in various parts. Sore, worse swallowing liquids. Septic parotiditis. Dry, intensely swollen, externally and internally. Diphtheria; membrane dusky, blackish; pain aggravated by hot drinks; chronic sore throat, with much hawking; mucus sticks, and cannot be forced up or down. Very painful; worse slightest pressure, touch is even more annoying – bleeds. Tonsils purplish. Purple, livid color of throat. Feeling as if something was swollen which must be swallowed; worse, swallowing saliva or liquids. Pain into ear. Collar and neck-band must be very loose. Gums swollen, spongy, bleed. Tongue swollen, burns, trembles, red, dry and cracked at tip, catches on teeth. Aphthous and denuded spots with burning and rawness. Nauseous taste. Teeth ache, pain extends to ears. Pain in facial bones. Bleeding, nostrils sensitive. Coryza, preceded by headache. Hay asthma; paroxysms of sneezing.
Belladonna
Diphtheria, throat dry, as if glazed; angry-looking congestion, red. Tonsils enlarged; throat feels constricted; difficult deglutition; worse, liquids. Sensation of a lump. Esophagus dry; feels contracted. Spasms in throat. Continual inclination to swallow. Scraping sensation. Muscles of deglutition very sensitive. Hypertrophy of mucous membrane.
Drying in nose, fauces, larynx, and trachea. Tickling, short, dry cough. Larynx feels sore. Respiration oppressed, quick, unequal. Cheyne-Stokes respiration. Hoarse; loss of voice. Barking cough, whooping cough, with pain in stomach before attack, with expectoration of blood. Stitches in chest when coughing. Larynx very painful. High, piping voice. Moaning at every breath. Violent palpitation, reverberating, labored breathing. Palpitation from least exertion. Throbbing all through body. Heart seemed too large. Rapid but weakened pulse.
Imaginary odors. Bleeding of nose, with red face. Coryza; mucus mixed with blood. Mouth dry. Throbbing pain in teeth. Gumboil. Tongue red on edges. Strawberry tongue. Grinding of teeth. Tongue swollen and painful. Stammering.
Natrum Muriaticum 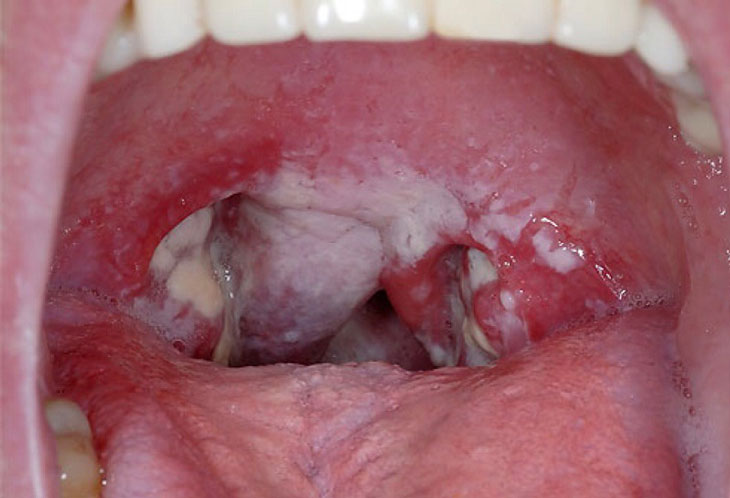
Dry mucous membranes. Constrictive throat. Hyperthyroidism/Goitre. Addison’s disease. Cough from a tickling in the pit of stomach, accompanied by stitches in liver and spurting of urine. Stitches all over chest. Cough, with bursting pain in head. Shortness of breath. Whooping-cough with flow of tears. Frothy coating on tongue, with bubbles on side. Numbness, tingling of tongue, throat, lips, and nose. Vesicles and burning on tongue. Tongue mapped. Loss of taste. Violent, fluent coryza. Discharge thin and watery, raw egg like. Violent sneezing coryza. Infallible for stopping a cold commencing with sneezing. Use thirtieth potency. Loss of smell and taste. Internal soreness of nose. Dryness.
Botulinum
Septicemia. Diphtheria. Difficulty in swallowing and breathing, choking sensation; weakness and uncertainty in walking, “blind staggers”, dizziness, thickening of speech. Cramping pain in stomach. Mask-like expression of face, due to weakness of facial muscles. Ptosis, double vision, blurred vision. Severe constipation.
P. S: This article is only for doctors having good knowledge about Homeopathy and allopathy, for learning purpose(s).
For proper consultation and treatment, please visit our clinic.
None of above-mentioned medicine(s) is/are the full/complete treatment, but just hints for treatment; every patient has his/her own constitutional medicine.
 Dr Qaisar Ahmed – Gastroenterologist, Specialist Homeopathic Medicines.
Dr Qaisar Ahmed – Gastroenterologist, Specialist Homeopathic Medicines.
Senior research officer at Dnepropetrovsk state medical academy Ukraine.
Location: Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Find more about Dr Sayed Qaisar Ahmed at:
https://www.youtube.com/Dr Qaisar Ahmed
Just wanna remark on few general things, The website pattern is perfect, the subject matter is real superb. “We can only learn to love by loving.” by Iris Murdoch.