
Sexual Pain or Dyspareunia or in other words Painful coitus.
The medical term for sexual pain or dyspareunia or painful intercourse or painful coitus is dyspareunia. This definition includes recurrent or persistent discomfort that happens before, during, or after intercourse.
Sexual pain or dyspareunia is a complex disorder that can be further classified as superficial or deep, and primary or secondary.
Superficial dyspareunia is pain localized to the vulva or vaginal entrance, and deep sexual pain or dyspareunia or dyspareunia is pain perceived inside the vagina or lower pelvis, which is often associated with deep penetration.
Primary sexual pain or dyspareunia occurs at initial intercourse, and secondary dyspareunia occurs after some time of pain-free intercourse.
Painful intercourse or sexual pain or dyspareunia is sometimes further characterized as vulvodynia. Vulvodynia is a chronic pain that is defined as genital pain with no known etiology that lasts more than three months and may or may not be associated with sexual intercourse.
The International Society for the Study of Vulvovaginal Diseases (ISSVD), the International Society for the Study of Women’s Sexual Health (ISSWSH), and the International Pelvic Pain Society (IPPS) further describe vulvodynia by the site of pain (localized, generalized, or mixed); if it is provoked, spontaneous, or mixed; or if the pain is intermittent, persistent, constant, immediate, or delayed.
Localized vulvodynia refers to pain limited to the vulvar vestibule around the hymeneal ring at the entrance to the vagina, and generalized vulvodynia is defined as pain affecting the entire vulvar region.
Vulvodynia has no clear etiology. However, ISSVD, ISSWSH, and IPPS list the following potential associated factors: other pain syndromes, genetics, hormonal factors, inflammation, musculoskeletal or neurologic mechanisms, psychosocial factors, and structural defects.
Dyspareunia and vulvodynia are often used interchangeably; however, it is important to appreciate that the terms have different meanings.
Sexual pain or dyspareunia is a descriptive term for the symptom of pelvic or vaginal pain associated with intercourse (i.e., it describes pain that always occurs with provoking touch such as intercourse). However, vulvodynia may occur with or without provocation (i.e., spontaneously). Dyspareunia can occur at the entrance of the vagina, deep in the vaginal canal, or in the pelvis.
Vulvodynia is localized to the vulva and vaginal introitus. Lastly, whereas dyspareunia may be acute or chronic, vulvodynia is a term used specifically for the classification of chronic pain (i.e, pain lasting longer than three months).
Both terms can be used to describe pain that coexists with other comorbidities such as endometriosis, interstitial cystitis, pelvic floor myalgias, and vulvar dermatoses.
Etiology and risk factors of Sexual Pain or Dyspareunia and vulvodynia
Sexual pain or dyspareunia is believed to be a specific pain disorder with interdependent psychological and biological etiologies. Like vulvodynia, superficial dyspareunia can be associated with vaginitis, dermatosis, and vulvovaginitis.
In contrast, deep sexual pain or dyspareunia can result from visceral disorders such as interstitial cystitis pelvic inflammatory disease, endometriosis, adhesions, pelvic congestion, and fibroids.
Pain syndromes can potentially overlap and be associated with dyspareunia and vulvodynia, including irritable bowel syndrome, fibromyalgia, and musculoskeletal dysfunction.
Other conditions that may contribute to the development of dyspareunia include poor vaginal lubrication, vaginal atrophy, and childbirth.
Childbirth is a risk factor for developing pelvic pain and/or dyspareunia during and potentially beyond the postpartum period.
A cross-sectional study on the effects of childbirth on sexual health reported that an estimated 17% to 36% of women reported dyspareunia at six months postpartum, yet only 15% of women who had postnatal dyspareunia discussed it with a health provider.
Associated comorbidities that may cause vulvodynia are vulvar/vaginal infections, inflammation, neoplasms, trauma, iatrogenic or hormonal deficiencies, neuropathic pain or pelvic floor muscle dysfunction, structural defects, and psychosocial factors.
Physical Exam for Sexual Pain or Dyspareunia
It is helpful to begin the physical inspection by first educating the patient about the examination and her anatomy while explaining what information has been obtained from each step of the assessment. 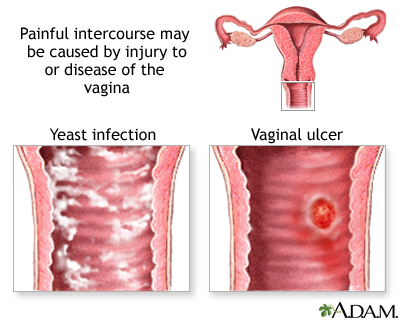
Physical examination of patients with genital pain should include an external musculoskeletal evaluation, followed by external visual and sensory examination, as well as internal single digit palpation of the pelvic floor muscles.
If tolerated by the patient, the provider may proceed to a bimanual examination and a speculum exam. It is important to recognize the possible discomfort and anxiety associated with assessments of the pelvis, particularly in patients with pain.
A common strategy used to minimize anxiety and discomfort is the interactive educational pelvic examination process, which includes:
1) explanations to the patient while performing the assessment.
2) describing the specific actions during each step.
3) using a mirror to enable the patient to visualize her anatomy and the examination. This allows the clinician to thoroughly evaluate the patient’s pain, exclude diagnoses, educate the patient regarding normal anatomy and sexual function, and reassure the patient when no pathology is uncovered.
The external musculoskeletal examination includes a complete lower back, abdomen, and pelvic inspection. It begins by observing any asymmetry or pain in the patient’s gait and her posture in the standing and sitting positions.
Next, the abdominal, gluteal, back, and lower extremity muscles are palpated to identify areas of tension and/or pain. Last, an assessment of muscle strength, range of motion, sensation, and reflexes should be performed.
The vulvar examination is performed systematically by inspecting the external genitalia, perineum, perianal areas, and mons pubis, and assessing for the presence of infection, trauma, atrophy, fissure, and dermatosis.
The standard test for diagnosis of vulvodynia is the cotton swab test. This test can help determine the location of pain as well as distinguish between mechanical allodynia and hyperalgesia.
- Allodynia is a term used to describe a painful response to a non-painful stimulation, such as light touch with a cotton swab.
- Hyperalgesia is an excessively painful response to a painful stimulus. The examiner can use the cotton-tipped applicator technique to conduct a sensory exam of the vulva and the six anatomical sites on the vestibule.
The clock face is used as a reference when describing the location of the vulva and pelvic structures. The 12 o’clock and six o’clock correspond to the anterior and posterior midline or pubic symphysis and anus, respectively.
The presence of allodynia or hyperalgesia on the vestibule is abnormal and suspicious for neuropathy.
The internal musculoskeletal and vaginal single-digit exam is the most reliable method for evaluating pelvic muscle tenderness.
Using the index finger, the examiner can palpate the lateral, anterior, and posterior walls of the vagina, the urethra, and pelvic floor muscles (levator ani, coccygeus, piriformis, and obturator internus).
The purpose is to access the specific areas for tone, tenderness, or involuntary spasms of the muscles of the introitus and pelvic floor.
Tenderness during minimal or moderate palpation is considered abnormal; pelvic and vaginal structures can tolerate approximately 2 kg of pressure without pain. The patient is then asked to squeeze or contract around the single digit to assess their muscle strength. An effort should also be made to identify any scars from previous surgeries, episiotomy, or trauma.
If the patient can tolerate the single digit muscular exam, a bimanual exam can be performed to evaluate the uterus and adnexa.
The purpose is to assess the uterus, cul-de-sac, and adnexa regions for any masses or tenderness. If the patient tolerates this portion of the exam, then the provider can proceed to an internal examination using a small-sized Grave’s or Pederson speculum.
All efforts should be made to insert the speculum slowly to allow accommodation of the speculum and to avoid touching the urethra or vulvar vestibule which can elicit pain.
During the speculum exam, the internal vaginal tissue, cervix, and vaginal secretions are examined. At this time, cultures or biopsies can be collected to rule out infections, dermatoses, or abnormal cellular dysplasia that can cause dyspareunia or vulvodynia.
Differential diagnosis
- Sexual pain or dyspareunia disorder: persistent recurrent genital pain or nonorganic cause associated with sexual stimulation.
- Vaginismus: painful, involuntary spasm of the vagina, preventing intercourse
- Vulvar vestibulitis: a chronic and persistent clinical syndrome characterized by severe pain with vestibular touch or attempted vaginal entry, tenderness in response to pressure within the vulvar vestibule, and physical findings confined to various degrees of vestibular erythema.
- Vulvodynia: chronic vulvar discomfort (e.g. burning, stinging, irritation, rawness).
- Female sexual dysfunction (disorders of desire, arousal, or orgasm)
Allopathic treatment for Sexual Pain or Dyspareunia
Current allopathic treatment recommendations for sexual pain or dyspareunia, and vulvodynia vary. The selected treatment should be specific if a cause is identified (e.g., vaginal infection, musculoskeletal, endometriosis).
Because vulvodynia is chronic genital pain, medical treatment for vulvodynia may be more challenging.
Homeopathic treatments should be individualized, and a multimodal treatment approach to address all aspects of pain (i.e., physical, emotional, and behavioral) is recommended.
Both sexual pain or dyspareunia and vulvodynia treatment plans, if appropriate, should start with conservative medical non-invasive approaches.
In allopathic way of treatment sometimes it is necessary to escalate to surgical interventions. This may involve a team approach with gynecology, physical therapy, pain management, sexual therapy, and mental health professionals who specialize in chronic pain.
Hormonal Treatment for Sexual Pain or Dyspareunia
Vulvovaginal atrophy caused by decreased levels of estrogen is a common problem in aging women. In patients who present with the main symptoms of atrophy, dryness, and dyspareunia, the first line of therapy consists of topical estrogen to restore normal vaginal pH levels and thicken and increase cell numbers leading to the revascularization of the epithelium.
Low-dose allopathic conjugated estrogens available in the forms of vaginal inserts (e.g., cream, tablet, and ring) can be applied periodically from a few times a week to every three months.
Topical estrogen should be considered to avoid the systemic effect of oral estrogen. However, patients using allopathic estrogen supplementation in any form should be followed clinically, and estrogen supplementation is contraindicated in patients with certain comorbidities such as breast cancer and uncontrolled cardiovascular disease. Additionally, topical vaginal estrogen therapy may take up to four weeks before patients notice an effect.
Anti-Inflammatory Agents
Tissue levels of interleukin B, an inflammatory mediator cytokine, have been reported to be higher in the hymenal region of the vestibule of women with vulvodynia.
Injectable anti-inflammatory agents such as corticosteroids, interferons, and mast cell stabilizers have been used to treat vulvodynia with some improvement. However, randomized controlled trials to recommend them as a first-line treatment are lacking.
Botulinum Type A
Allopathic injection of botulinum toxin A into the pelvic floor muscles has been shown in some studies to decrease dyspareunia and vulvodynia caused by pelvic floor myalgia and contracture.
Botulinum toxin A is hypothesized to inhibit nociceptors leading to a decrease in peripheral and central sensitization associated with vulvodynia.
A long-term assessment of the effectiveness of botulinum injections after 24 months revealed that patients could have sexual intercourse and had improved quality of life.
It is not recommended as a first-line therapy as further clinical trials of botulinum type A are needed, but it is used as an adjunct to other therapies.
Systemic Medications
Tricyclic antidepressants and anticonvulsants have been shown to improve pain symptoms in patients with vulvodynia.
Tricyclic antidepressants such as amitriptyline are known to reduce peripheral nerve sensitization and have been used in the management of neuropathic pain. It can take up to three weeks to achieve pain control.
Although patients have reported symptomatic relief from vulvodynia with tricyclic pharmacotherapy, additional research is required for allopathic researchers to identify the characteristics that would predict the appropriate patients for this therapy.
Surgical Therapy for Sexual Pain or Dyspareunia
Surgical treatment is performed as a last resort for allopath when all conservative and medical management options have failed or when surgery is indicated to determine and/or treat pelvic adhesions, endometriosis, or pelvic organ prolapse.
The surgical options are specific to the disorder, but most commonly include vulvar vestibulectomy, lysis of pelvic adhesions, or excision of endometriosis.
Thorough counseling is necessary prior to pursuing surgical treatment. Patients must understand that surgery may improve their pain, but their pain may sometimes return or worsen.?
Vestibulectomy can be an effective treatment only for localized, provoked vestibulodynia.
Generally, surgical techniques include a complete vulvar vestibulectomy, which involves excision of the mucosa of the entire vulvar vestibule and the mucosa adjacent to the urethra, or a modified vestibulectomy, which limits the excision of mucosa to the posterior vestibule.
Homeopathic Treatment for Sexual Pain or Dyspareunia

There are plenty of medicines in Homeopathy for the treatment of sexual pain or dyspareunia, for example:
Platina
Parts hypersensitive. Tingling internally and externally. Ovaries sensitive and burn. Menses too early, too profuse, dark-clotted, with spasms and painful bearing-down, chilliness, and sensitiveness of parts. Vaginismus. Nymphomania. Excessive sexual development; vaginismus. Pruritus vulvae. Ovaritis with sterility. Abnormal sexual appetite and melancholia.
Origanum Majorana
Erotomania; powerful lascivious impulses; leucorrhea; hysteria. Lascivious ideas and dreams.
Kali Bromatum
Pruritus. Ovarian neuralgia with great nervous uneasiness. Exaggerated sexual desire. Cystic tumors of ovaries.
Belladonna
Sensitive forcing downwards, as if all the viscera would protrude at genitals. Dryness and heat of vagina. Dragging around loins. Pain in sacrum. Menses increased, bright red, too early, too profuse. Hemorrhage hot. Cutting pain from hip to hip. Menses and lochia very offensive and hot. Labor-pains come and go suddenly. Mastitis pain, throbbing, redness, streaks radiate from nipple. Breasts feel heavy; are hard and red. Tumors of breast, pain worse lying down. Badly smelling hemorrhages, hot gushes of blood. Diminished lochia.
Thuja Occidentalis
Vagina very sensitive. Warty excrescences on vulva and perineum. Profuse leucorrhea; thick, greenish. Severe pain in left ovary and left inguinal region. Menses scanty, retarded. Polypi; fleshy excrescences. Ovaritis; worse left side, at every menstrual period (Lach). Profuse perspiration before menses.
Caulophyllum
Extraordinary rigidity of os. Spasmodic and severe pains, which fly in all directions; shivering, without progress; false pains. Revives labor pains and furthers progress of labor. After pains. Leucorrhea, with moth-spots on forehead. Habitual abortion from uterine debility (Helon; Puls; Sab). Needle-like pains in cervix. Dysmenorrhea, with pains flying to other parts of body. Lochia protracted, great atony. Menses and leucorrhea profuse.
Coffea Cruda
Menses too early and long lasting. Dysmenorrhea, large clots of black blood. Hypersensitive vulva and vagina. Voluptuous itching.
Ignatia Amara
Menses black, too early, too profuse, or scanty. During menses great languor, with spasmodic pains in stomach and abdomen. Feminine sexual frigidity. Suppression from grief. 
Murex Purpurea
Conscious of a womb. Pulsation in neck of womb. Desire easily excited. Feeling as if something was pressing on a sore spot in the pelvis: worse sitting. Pain from right side of womb to right or left breast. Nymphomania. Least contact of parts causes violent sexual excitement. Sore pain in uterus. Menses irregular, profuse, frequent, large clots. Feeling of protrusion. Prolapse; enlargement of uterus, with pelvic tenesmus and sharp pains, extending toward breasts; aggravated lying down. Dysmenorrhoea and chronic endometritis, with displacement. Must keep legs tightly crossed. Leucorrhoea green or bloody, alternate with mental symptoms and aching in sacrum. Benign tumors in breasts. Pain in them during menstrual period.
Magnesium Phosphoricum
Menstrual colic. Membranous dysmenorrhoea. Menses too early, dark, stringy. Swelling of external parts. Ovarian neuralgia. Vaginismus.
Staphysagria
Parts very sensitive, worse sitting down. Irritable bladder in young married women. Leucorrhoea. Prolapsus, with sinking in the abdomen; aching around the hips.
Berberus Vulgaris
Pinching constriction in mons veneris, vaginismus, contraction and tenderness of vagina. Burning and soreness in vagina. Desire diminished, cutting pain during coition. Menses scanty, gray mucus, with pain in kidneys and chilliness, pain down thighs. Leucorrhoea, grayish mucus, with painful urinary symptoms. Neuralgia of ovaries and vagina.
Lyssinum
Uterine sensitiveness; conscious of womb. Feels prolapsed. Vagina sensitive, rendering coition painful. Uterine displacements.
Helonias Dioica
Dragging in sacral region, with prolapse, especially after a miscarriage. Pruritus vulvae. Backache after miscarriage. Weight and soreness in womb; conscious of womb. Menses too frequent, too profuse. Leucorrhoea. Breasts swollen, nipples painful and tender. Parts hot, red, swollen; burn and itch terribly. Albuminuria during pregnancy. Debility attending the menopause.
Conium Maculatum
Dysmenorrhoea, with drawing-down thighs. Mammae lax and shrunken, hard, painful to touch. Stitches in nipples. Wants to press breast hard with hand. Menses delayed and scanty; parts sensitive. Breasts enlarge and become painful before and during menses. Rash before menses. Itching around pudenda. Unready conception. Induration of os and cervix. Ovaritis; ovary enlarged, indurated; lancinating pain. Ill effects of repressed sexual desire or suppressed menses, or from excessive indulgence. Leucorrhoea after micturition.
Nux vomica
Menses too early, lasts too long; always irregular, blood black with faint spells. Prolapsus uteri. Dysmenorrhoea, with pain in sacrum, and constant urging to stool. Inefficient labor-pains; extend to rectum, with desire for stool and frequent urination. Desire too strong. Metrorrhagia, with sensation as if bowels wanted to move.
Nitric Acid
External parts sore, with ulcers (Hep.: Merc; Thuja). Leucorrhoea brown, flesh-colored, watery, or stringy, offensive. Hair on genitals falls out. Uterine haemorrhages. Menses early, profuse, like muddy water, with pain in back, hips and thighs. Stitches through vagina. Metrorrhagia after parturition.
Sepia
Sepia is a very beneficial medicine for treating dyspareunia. Pelvic organs relaxed. Bearing down sensation, Leucorrhoea yellow, greenish; with much itching. Menses Too late and scanty, irregular; early and profuse; sharp clutching pains. Violent stitches upward in the vagina, from uterus to umbilicus. Prolapse of uterus and vagina. Morning sickness. Vagina painful, especially on coition.
Intense pain during intercourse, vaginal dryness, vaginal extremely tender.
There may be some associated pelvic disease like ovarian cysts, uterine fibroids pelvic inflammatory disease (PID) and endometriosis.
In such conditions, other symptoms like abnormal vaginal discharge, menstrual irregularities, painful periods may be present along with dyspareunia.
Sepia is also a leading medicine for managing the complaint of painful intercourse in women during menopause. Inmenopausall patients there may be other attending symptoms like hot flushes, excessive vaginal bleeding, low libido, irritability, sadness, indifference, and mood swings during menopause.
It is also well-indicated for dyspareunia arising with some skin infection or eruptions of the female genitalia.
Natrum Mur
Natrum Mur is very beneficial to treat cases of painful intercourse from dryness of the vagina. Pressure and general bearing down towards genital organs every morning, vagina is also sore and itchy. Burning and smarting are felt in the vagina during coition along with pain. Prolapsus uteri with aching in loins.
Catamenia premature and profuse; or retarded and scanty.-Sterility, with too early and too profuse menstruation. Itching in genital organs. Repugnance to coition, Coition: painful from dryness of vagina; burning smarting during; in anaemic women with dry mouth and dry skin.
Leucorrhoea, with headache, disposition to diarrhoea, colic, and mucous evacuations. Acrid (greenish) leucorrhoea (increased discharge when walking), with pale face. Abundant discharge of transparent, whitish, and thick mucus from vagina.
Vulvitis with falling off of hair. Itching of external parts with falling off of hair. Pimples on mons veneris.
Nausea and vomiting during pregnancy; morning sickness with vomiting of frothy, watery phlegm.
During pregnancy: dysuria; albuminuria; craves salt; congestion to chest; palpitation; haemorrhoids; cough; escape of urine.
Labour slow, pains feeble, apparently from sad feelings and forebodings.
Lancinating pains in breasts. Stitches beneath nipples.Dull stitch beneath right nipple in abdomen. Breasts sensitive to slightest touch.
Aversion to sexual intercourse. There may be some depression or history of grief present in cases needing Natrum Mur.
Platina
Sensitive, tender vagina – cannot bear to touch it. They may even faint during coition. In many cases, there may be vaginismus that makes intercourse impossible. Pains of drawing nature may appear in the ovaries and uterus after intercourse that tend to last for several hours altogether. Sensation of bearing down towards genital organs, with aching in abdomen.
Unnatural increase of sexual desire, with painful sensibility and voluptuous tingling from genitals up into abdomen. Nymphomania, which may occur even during the period. Induration of uterus. Sanguineous congestion in uterus. Miscarriage. Metrorrhagia (with great excitability of the sexual system) of thick, deep-coloured blood, with drawings in groins.
Catamenia too early and too profuse (blood dark and coagulated), sometimes with headache, restlessness, and tears. Menstruation, when the discharge is very abundant, thick and black like tar, and is very exhausting; spasms and screaming at every menstrual period. Catamenia too long continued. Before catamenia, cuttings and pains like those of labour in hypogastrium.
Cramps at commencement of catamenia. Painful sensitiveness and constant pressure in mons veneris and genital organs, with internal chill and external coldness, except face. Severe stitches in r. ovarian region. During catamenia, pressure as of a general bearing down towards genital organs, which are very sensitive.
Leucorrhoea, like white of eggs, flowing chiefly after urinating, and on rising from a seat.
Argentum Nitricum
Argentum Nitricum is considered in cases of dyspareunia when painful intercourse is followed by vaginal bleeding, vaginal discharge with cervical erosions, vaginal discharges are profuse, yellow, corroding; they may be bloodstained.
Ovarian pains, feels as if an enormous swelling inside affected. Prolapsus with ulceration of os or cervix; with copious yellow, corroding leucorrhea and frequent bleeding from points of ulceration. Sexual pain or dyspareunia.
Menses irregular; scanty (with asthma). Menses too copious or too scanty, too soon or too late. All symptoms better before and during menses.
Coition painful, followed by bleeding from the vagina. Orgasms at night. Metrorrhagia, Metrorrhagia, with nervous erethism at change of life also, in young widows and those who have borne no child; returning in attacks, region of ovaries painful, with pains radiating to sacrum and thighs.
During pregnancy, stomach as if it would burst with wind; head feels expanded. Puerperal convulsions; just after attack lies quiet but becomes very restless before another.
Staphysagria
Nymphomania, with extreme sensitiveness to mental and physical impressions; mind dwells too much on sexual subjects. Painful sensitiveness of genital organs (especially when sitting). Prurigo senilis; or from pediculi. Smarting and lancinating itching in vulva. Sufferings after coitus in newly married women. Sexual pain or dyspareunia.
Inflammation of the ovaries with burning, stinging, and pressing-drawing, very sharp shooting pains in ovary – exceedingly sensitive to pressure; pains extending into crural region and thighs. Flow of blood from genitals a long time after critical age.
Menses which had ceased for a year, reappeared with cutting colic and violent rumbling, at the new moon. Spasmodic pains in vulva and vagina. Menses: irregular, late, and profuse; sometimes wanting; first of pale blood, then dark and clotted; occasionally spasmodic uterine contractions. Amenorrhea from chagrin with indignation. Granular vegetations of vagina.
Kreosotum Sexual Pain or Dyspareunia
Premature catamenia, of too long and too copious continuance with a discharge of black blood. During an embrace, burning in the parts, followed next day by menstrual discharge of dark blood.
Appearance of menses in third month of pregnancy (blood black, flows in a stream). Before the catamenia, abdominal spasms, leucorrhea, irritation, and inquietude, vomiting of mucus or frothy risings, and inflation of the abdomen. During menses: Hardness of hearing; discharge of fetid wind, constipation, and incarceration of flatus; buzzing and roaring in head; with pressive pains, colic, cuttings, sacral pains, constant shivering, or sweat on the back, and on the chest.
After menses: Abdominal spasms; pressure in the genitals; leucorrhea; and many other sufferings. Pains during menses but better after. Menses flow only when lying down, cease on sitting or walking.
Metrorrhagia better by lying while worse getting up and walking. Metrorrhagia; in fungoid disease of endometrium. Sexual pain or dyspareunia.
Leucorrhea, corrosive or mild, and sometimes followed by exhaustion and fatigue, especially in legs. Leucorrhea of a yellow color, staining linen yellow, with great weakness in legs. White leucorrhea, having odor of green corn.
Nausea during pregnancy; ptyalism; excoriating lochia. Dwindling away of mammae, with small, hard, painful lumps in them.-Leucorrhea putrid, with accompanying complaints; leucorrhea in general, esp. if very fetid and exhausting.-Complaints of females at change of life.-Cramp-like pains in external genitals.-Excoriation, with smarting pains between genitals and thighs.-Shootings in vagina, as if produced by electricity.-Voluptuous itching in vagina.-Itching in vagina, inducing rubbing in evening, succeeded by smarting, swelling, heat, and induration of external parts, with soreness in vagina when urinating.-Desire for coition, in females, esp. in morning.-After coition, pain, as of excoriation, and hard knottiness in neck of uterus, or swelling of the genital parts (both male and female) with burning pains (worse in morning than in evening).-After coition discharge of dark blood the next day.-Prolapsus vaginae. Prolapsus uteri. Pulling, stitches, and shootings in the mammary glands.
Ignatia
Catamenia premature and violent, every ten or fifteen days, Blood of the catamenia black, of putrid odor, mixed with clots. During the catamenia, heaviness, heat, and pain in the head, photophobia, colic, and contractive pains, anxiety, palpitation of the heart, and great fatigue, even to fainting, Cramp in the uterus, during the catamenia.
Metrorrhagia. Cramp-like and compressive pains in the region of the uterus, with fits of suffocation; pressure, and lying on the back, mitigate the pain. Uterine spasms, with lancinations, or like labor pains. Sexual pain or dyspareunia.
Corrosive and purulent leucorrhea, preceded by contractive pressure in the uterus, extreme sore pain in the vagina during intercourse. A heated sensation may be present in the vagina.
Sadness, weeping, excessive irritability, desire for loneliness, aversion to talking and sudden mood swings. Excessive worries, depression, and history of grief may be there with the above symptoms.
Lycopodium Clavatum
Nymphomaniac with terrible teasing desire in external organs. Itching, burning, and gnawing in vulva. Pressure towards the outside, above the vulva, and extending as far as the vagina, when stooping. Sexual pain or dyspareunia.
Expulsion of wind from the vagina. Chronic dryness of vagina. Shooting pains in labia, when lying down. Excoriation between the thighs, and at the vulva. Burning pain in the vagina, during and after coition.
Catamenia (too early) too profuse, and of too long duration. Catamenia suppressed readily, and for a long time, by fright. Before menses: shivering, sadness, melancholy; bloatedness of the abdomen.
During menses: delirium, with tears; headache; sourness in the mouth; pain in loins; swelling of feet; fainting; vomiting of sour matter; cuttings, colic; and pains in the back. Menstruation too late; lasts too long; sometimes suppression of; profuse, protracted; flow partly black, clotted, partly bright red or partly serum; with labor-like pains followed by swooning; with sadness; suppressed by fright.
May find females at change of life with one side of the body greatly hypertrophied. Fetus appears to be turning summersaults. Metrorrhagia; at menopause; dark blood with large clots pours from her. A rumbling begins in upper abdomen and descends to lower, when a flow of blood follows, and so on successively.
Leucorrhea: milky, yellowish, reddish, and corrosive; sometimes preceded by cuttings in abdomen. Varices on the genitals. Disposition to miscarriages. Swelling of the breasts with nodosities. Excoriation and moist scabs on nipples. Stinging in nipples. Milk in breasts without being pregnant, vaginl dryness.
P. S: This article is only for doctors having good knowledge about Homeopathy and allopathy, for learning purpose(s).
For proper consultation and treatment, please visit our clinic.
None of above-mentioned medicine(s) is/are the full/complete treatment, but just hints for treatment; every patient has his/her own constitutional medicine.
To order medicine by courier, please send your details at WhatsApp– +923119884588
 Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Senior research officer at Dnepropetrovsk state medical academy Ukraine.
Location: Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Find more about Dr Sayed Qaisar Ahmed at:
https://www.youtube.com/Dr Qaisar Ahmed
https://www.facebook.com/ahmed drqaisar
Pretty nice post. I just stumbled upon your weblog and
wished to say that I have truly enjoyed surfing around your blog
posts. In any case I’ll be subscribing to your
feed and I hope you write again soon.
I’m now not positive the place you’re getting your info, however good topic.
I needs to spend a while finding out much more or understanding more.
Thank you for great info I was in search
of this info for my mission.
I’ve been surfing online more than 3 hours today, yet I never found any interesting article like
yours. It is pretty worth enough for me. Personally, if
all website owners and bloggers made good content as you did, the web will be a lot
more useful than ever before.
What’s up friends, how is everything, and what you want to say regarding
this article, in my view its genuinely amazing for me.
Everyone loves it whenever people get together and share views.
Great website, stick with it!
Its not my first time to pay a quick visit this website, i am visiting this web page dailly and obtain good information from here all the time.
I don’t even know how I ended up here, but I thought this post was good.
I do not know who you are but certainly you’re going to a famous
blogger if you are not already 😉 Cheers!
Hi, after reading this amazing piece of writing i am too glad to
share my familiarity here with colleagues.
Superb blog! Do you have any helpful hints for aspiring writers?
I’m planning to start my own website soon but I’m
a little lost on everything. Would you recommend starting with a free platform like WordPress or go for a paid option?
There are so many choices out there that I’m totally overwhelmed ..
Any suggestions? Kudos!
I’m gone to say to my little brother, that he should
also visit this web site on regular basis to get updated from hottest reports.
Ahaa, its good dialogue on the topic of this piece of writing here at this website, I
have read all that, so now me also commenting here.
Somebody necessarily lend a hand to make seriously posts I would
state. That is the first time I frequented your website page and so far?
I surprised with the research you made to make this actual publish incredible.
Fantastic job!
fantastic issues altogether, you just won a new reader.
What might you suggest about your put up that you just made some
days in the past? Any certain?