
Human papillomavirus (HPV) is the most common sexually transmitted infection. Human papillomavirus (HPV) produces epithelial tumors of the skin and mucous membranes. HPV infections and the development of warts are common throughout life if not treated with Homeopathy. Generally, genital HPV infection is considered to have become significantly more frequent over the past several decades.
The current classification system for HPV, which is based on similarities in genomic sequences, generally correlates with the 3 clinical categories applied to HPV infection: 
-
Anogenital or mucosal (further subclassified as latent [asymptomatic], subclinical, or clinical),
-
Non genital cutaneous,
-
Epidermodysplasia verruciformis.
Human papillomavirus (HPV). Verrucae and papillomas appear as frondlike epithelial proliferations. Verrucae tend to be more keratinized with sharper projections than papillomas.
Human papillomavirus (HPV). Verruca vulgaris on the lateral border of the tongue exhibits the multiple, sharp-tipped, white, verrucous appearance, which is
 classic for this lesion in the oral cavity. Not all verrucae are so clinically diagnostic. Courtesy of Rose Yin Geist, DDS.
classic for this lesion in the oral cavity. Not all verrucae are so clinically diagnostic. Courtesy of Rose Yin Geist, DDS.
Other Cancers
The percentages of other cancers caused by oncogenic HPV are as follows:
-
Anal cancer: 90%,
-
Vulvar cancer: 40%,
-
Vaginal cancer: 40%,
-
Oropharyngeal cancer: 12%,
-
Oral cancer: 3%.
Background
HPV produces epithelial tumors of the skin and mucous membranes. There are over 100 known HPV types, with genomes of more than 80 fully sequenced. Individuals with multiple sexual partners or persistent HPV infections are at higher risk of acquiring additional HPV strains. The current classification system, based on genomic similarities, generally corresponds to three clinical categories of HPV:
- Anogenital or mucosal,
- Nongenital cutaneous,
- Epidermodysplasia verruciformis (EV).
Mucosal HPV (anogenital)
Mucosal HPV infections are classified as latent (asymptomatic), subclinical, or clinical. Clinical lesions are visibly apparent, whereas latent infections are detectable only through viral DNA tests. Subclinical lesions are identified using 3-5% acetic acid and magnification. Most HPV infections are latent; clinically visible infections typically manifest as warts rather than malignancies.

Genital warts
HPV infections are common and result in various clinical manifestations on epidermal surfaces. Condylomata acuminata (genital warts) are benign proliferations of anogenital skin and mucosa caused by HPV infection. They are transmitted through sexual contact, with approximately two thirds of exposed individuals developing genital warts. The incubation period is estimated to be between 3 weeks and 8 months.
Although generally benign, certain HPV types can significantly increase the risk for anogenital cancer. Some types also are associated with laryngeal, oral, and certain lung cancers.
HPV types 6 and 11 typically are classified as low-risk due to their low oncogenic potential, often causing condylomata and low-grade precancerous lesions. HPV types 16 and 18 are considered high-risk as they are responsible for most high-grade intraepithelial lesions that may progress to carcinomas, particularly in anogenital or mucosal regions.
Alone HPV infection does not lead to malignant transformation of infected tissue. Co-factors such as tobacco use, radiation, allopathic medicines, folate deficiency, and immune suppression are implicated in this process.
Etiology
The definitive cause of anogenital warts is HPV infection. The HPV capsid lacks an envelope, which makes the organism very stable and resistant to various treatments. No serologic typing is available, because of the lack of consistent in vitro culture methods. Typing of HPV is based on genotype, which generally is determined by molecular hybridization using molecularly cloned HPV DNA of known type as the standard. Two HPV are of different types when their DNA hybridize (bind) less than 50% as efficiently to each other as to themselves.
The nearly 40 types of HPV that have been found in genital warts are highly host specific. These viruses do not infect laboratory animals. In addition, HPV types demonstrate a high degree of site specificity, with some types only found on certain parts of the skin or mucous membranes. As a rule, HPV types causing common warts of the skin do not infect moist epithelium, and vice versa.
Risk Factors
HPV infection alone does not directly cause malignant transformation of infected tissue. However, cofactors such as tobacco use, radiation, allopathic medicines, folate deficiency, and immune suppression have been implicated in this process, particularly in the anogenital-mucosal category. Patients receiving immunosuppressive drugs (allopathic) and those with defects in cell-mediated immunity, including those infected with HIV, are especially susceptible to HPV infections.
Sexual Activity
There is a direct correlation between anogenital HPV infection and measures of sexual activity, such as the age of first intercourse and the lifetime number of sexual partners. 
Women with a history of high-grade squamous intraepithelial lesions (HGSIL) of the cervix or invasive squamous cell carcinoma (SCC) of the cervix are at increased risk for subsequent development of invasive cancer in other tissues of the anogenital-mucosal category, particularly vaginal and anal carcinoma (relative risks of 5.6 and 4, respectively).
Anal cancer has been strongly associated with male homosexuality and specific male practices, such as engaging in receptive anal intercourse; the relative risk is 33. However, the overall disease prevalence is higher in women than in men, with a female-to-male ratio of 1.5:1.
Tobacco Smoking
Women who smoke tobacco have an increased risk of developing cervical neoplasia. Measurable amounts of potent carcinogens, as well as several compounds from cigarette smoke, have been identified in the cervical mucus of females who smoke. These agents likely contribute to the increased prevalence of HPV malignant transformation observed in tobacco users.
Oral Contraceptive Use
Women who take oral contraceptives (allopathic only) for longer than 2 years have an increased relative risk of developing breast cancer and cervical carcinoma. This risk will not decline even after discontinuation of oral contraceptive use. 
Chewing tobacco
A high incidence of oral cancer associated with HPV infection has been demonstrated in India among patients who chew tobacco. This stimulant, made from the leaves of the tobacco leave, is used similarly to sniffing tobacco.
Clinical Ultraviolet and x-ray radiation
Epidermodysplasia verruciformis (EV) is particularly susceptible to clinical/mechanical ultraviolet (UV) and x-ray radiation; therefore, patients with EV should avoid activities that unnecessarily expose them to these forms of radiation.
Signs and Symptoms
The clinical history and presentation of HPV infection vary depending on the anatomic area involved. The preference of certain viral genotypes for specific epidermal sites largely determines the areas of involvement. Conditions associated with HPV include the following: 
Anogenital warts (condylomata acuminata):
Cervical disease:
Anal cancer:
Nonanogenital mucosal disease:
Nongenital cutaneous disease:
Epidermodysplasia verruciformis.
Physical findings vary depending on the tissues involved and may include the following:
-
Typical condylomata: Discrete, papillary, cauliflower-like lesions involving multiple sites on moist surfaces.
-
Keratotic warts: Often seen on dry surfaces such as the labia majora.
-
Discrete papules: 1-3 mm in size can present on the shaft of the penis.
-
Cervical intraepithelial lesions: May be found upon examination of the cervix.
-
Subclinical infection: Tiny, slightly raised areas felt or visualized on the vagina or cervix.
History
The clinical history and presentation of human papillomavirus (HPV) infection vary according to the anatomic area involved. The predilection of certain virus genotypes to infect specific epidermal sites largely determines the areas of involvement.
Genital infection:
Genital infection manifests as warty lesions on the genital or anal area, although these warts often are not initially recognized. Cervical infection generally goes unnoticed and is discovered during cervical examination or Papanicolaou (Pap) testing. 
Anogenital warts:
Condylomata acuminata are exophytic, cauliflower-like lesions typically found near moist surfaces such as the perianal area, vaginal introitus, vagina, labia, and vulva. They also may appear on dry surfaces, such as the shaft of the penis.
Genital warts include smooth papular warts and keratotic warts, the latter resembling non-genital cutaneous warts due to their thickened, bumpy surface. Flat condylomata (squamous intraepithelial neoplasia) are the most common lesions of the cervix but also may develop on the vulva, anus, and male genitalia, appearing as white, plaque-like growths.
An additional malignant variant is the giant condyloma, or Buschke – Löwenstein tumor, generally regarded as a verrucous carcinoma. These most often involve the glans penis, perianal area, and foreskin. In addition to their large cauliflower shape, they tend to form abscesses and fistulas and invade locally.
Genital warts generally do not become clinically apparent until several months after inoculation with HPV. They follow a slow and indolent course and may develop by inoculation from opposing surfaces. Condyloma acuminata often are asymptomatic but can be associated with pruritus. Bleeding may occur if the lesions become confluent and are irritated by clothing. Most patients seek medical care when they notice lumps on the vulva, perianal area, or periclitoral area, or experience pruritus or occasional bleeding.
Cervical disease:
Most cervical infections either are latent or subclinical and therefore asymptomatic. These infections are detected on Pap smear and reported as either a low-grade squamous intraepithelial lesion (LGSIL) or a high-grade squamous intraepithelial lesion (HGSIL). Further examination with 3-5% acetic acid and colposcopy shows characteristic acetowhite changes and abnormal blood vessels indicative of HPV-triggered dysplasia.
Patients who have neglected annual Pap testing for several years or more and have an HGSIL that has progressed to invasive cervical cancer may report vaginal bleeding between periods or after sexual intercourse, dyspareunia, and fullness in the pelvis. 
Anal cancer:
The most common presenting symptoms of squamous cell carcinoma (SCC) of the anus are rectal bleeding and the sensation of a mass. These symptoms may be mistakenly attributed to hemorrhoids.
Fifty percent of men who are homosexual and have SCC of the anus have a history of anorectal warts; however, only 20% of women with SCC and men who are not homosexual have this history.
Nonanogenital mucosal disease:
Oral warts represent infection of the oral mucosa. Although they are subtle and easily missed, they are fairly common. HPV types 6 and 11 have been isolated from nonanogenital mucosal surfaces. Warts have been discovered in the nares, mouth, larynx, and conjunctiva.
HPV types 6 and 11 are associated with respiratory papilloma that probably are the result of intrapartum transmission when the infant passes through the birth canal of a mother who is infected with HPV. However, isolated case reports exist of respiratory papillomatosis after cesarean delivery. Patients with laryngeal papilloma most frequently present with hoarseness at an average age of 3 years.
Focal epithelial hyperplasia (Heck disease) is a disseminated HPV infection of the oral mucosa most commonly associated with HPV 32 and HPV 13. This condition may have a family predilection.
Nongenital cutaneous HPV:
Common cutaneous warts (verruca vulgaris) generally appear on keratinized skin, presumably at the site of inoculation. Autoinoculation from a wart on one finger may cause warts on an adjacent finger or other skin surface (so-called kissing warts).
Common cutaneous warts appear as circumscribed, rough, hyperkeratotic papulonodular or plaques with irregular scaly surfaces and develop most often on the hands, fingers, feet, and knees. Such warts frequently are discovered when the patient notices changes in the skin. In general, they are asymptomatic, but they may be painful with the application of pressure. Typically, they are benign and self-limited.

Palmoplantar warts appear on the acral surfaces of the feet and hands. They are notable for their thickness, which complicates treatment. Deep plantar warts occur most commonly as solitary lesions that may become black and painful before spontaneously regressing. They may contain small black “seeds,” which are thrombosed capillaries.
Plantar warts
Flat warts (verruca plana) most often occur in groups of small plaques less than 5 mm in diameter on the face and hands. They often are not obvious but may induce significant disturbances of pigmentation. Regression usually occurs spontaneously after several years, and pruritus or erythema occurs several weeks before their disappearance.
Flat warts 
Malignant conversion of skin lesions
Malignant conversion of skin lesions typically begins in the fourth and fifth decades of life. Premalignant lesions usually arise first on the forehead and other sun-exposed areas. The tumors may be benign papilloma and seborrheic keratoses or premalignant actinic keratoses and squamous cell carcinoma (SCC).
Epidermodysplasia verruciformis
Epidermodysplasia verruciformis (EV) is an autosomal recessive familial trait that increases susceptibility to a subset of warts generally not observed in populations without EV. HPV genotypes associated with EV have been observed in patients who are immunosuppressed due to organ transplantation or HIV infection. These individuals are at increased risk for skin cancer if not recognized and treated.
EV generally begins in childhood and can affect almost any area of the body. The warts generally are subtle and flat and initially may be mistaken for tinea versicolor. EV tumors are locally destructive, develop slowly, and have weak metastatic potential if no cocarcinogens, such as x-ray or ultraviolet B irradiation, are applied. Polymorphic, plane wart-like, and red-to-brownish plaques can be distributed widely over the skin. The lymph nodes and oral mucosa are not involved.
Physical Examination
The physical examination findings depend on the tissues involved and include various cutaneous lesions with characteristic appearances (see History). 
Typical condylomata are discrete, papillary, cauliflower-like lesions that appear at multiple sites on moist surfaces. Keratotic warts often are observed on dry surfaces such as the labia majora. Warts vary in size and can develop into large, exophytic, cauliflower-like masses (see the images below). Discrete papules ranging from 1-3 mm in size can be present on the shaft of the penis. Growth can extend into the vagina, urethra, cervix, perirectal epithelium, anus, and rectum. Cervical intraepithelial lesions also may be identified upon examination of the cervix.
Human papillomavirus (HPV). Condyloma acuminatum in a patient with a history of an allograft renal transplant.
Human papillomavirus (HPV). Note the extensive labial involvement.
Human papillomavirus (HPV). Anal condyloma acuminatum.
Human papillomavirus (HPV). These condylomata extend to the anal verge.
Subclinical
Subclinical infection is another common presentation of condyloma. Tiny, slightly raised areas can be felt or visualized on the vagina or cervix. These flat warts are best visualized by using 3-5% acetic acid and a colposcope. Areas infected with HPV appear acetowhite (ie, white when “painted” with the acetic acid). Often, a biopsy is needed to distinguish these lesions from cervical squamous intraepithelial lesions or vaginal intraepithelial lesions.

The sexual partner or partners of a woman with condylomata should be examined by a physician and treated if indicated. Often, the examination of the male fails to reveal any visible condylomata.
Diagnosis
Diagnosis of most cutaneous and external genital warts typically can be achieved through clinical examination or by applying acetic acid and conducting a biopsy. In cases of genital intraepithelial neoplasia, it is crucial to assess the extent of the disease through meticulous inspection and colposcopy.
Laboratory studies that may be considered include the following:
-
Cervical cytologic testing with the Papanicolaou (Pap) test to screen for cervical neoplasia (current guidelines recommend delaying initiation and extending intervals between subsequent screens).
-
HPV DNA testing (eg, Hybrid Capture II or polymerase chain reaction [PCR] assay) for detecting HPV and post-treatment follow-up of cervical intraepithelial neoplasia.
The acetic acid test may be used in conjunction with colposcopy to examine suspicious cervical lesions, but it is not recommended for routine screening.
In certain cases, tissue biopsy may be necessary to confirm HPV infection. Biopsy is recommended in the following scenarios:
-
Women with a history of vulvar dysplasia.
-
Postmenopausal women.
-
Cases where medical therapy fails.
-
When there is clinical doubt about the diagnosis.
Histologic findings useful for diagnosing include:
-
Common cutaneous warts: Marked hyperkeratosis, acanthosis, parakeratosis, and papillomatosis. Koilocytes, vertical columns of parakeratosis, and foci of clumped keratohyalin granules distinguish warts from another papilloma.
-
Condyloma acuminatum: Epidermal disruption with hyperkeratosis, coarse keratohyalin granules, and koilocytes in a prominent granular layer. Flat condylomata exhibit acanthosis in the epidermis or mucosa.
Bowenoid papulosis: Psoriasiform hyperplasia and hyperkeratosis of the epidermis, increased mitotic figures at all epidermal levels, and keratinocytes with enlarged pleomorphic and hyperchromic nuclei.
Allopathic treatment for human papilloma virous
All allopathic medications used to treat HPV disease are applied topically and should not be applied to mucosal surfaces. Those allopathic medicines are not suitable for treating dysplastic lesions, squamous cell carcinoma, verrucous carcinoma, or Bowenoid papulosis.

Allopathic medications fall into the following two broad categories:
- Immune response modifiers: Examples include imiquimod and interferon alfa. These primarily are used for treating external anogenital warts or condylomata acuminata.
- Cytotoxic agents: These include antiproliferative drugs such as podofilox, podophyllin, and 5-fluorouracil (5-FU), as well as chemodestructive or keratolytic agents like salicylic acid, trichloroacetic acid (TCA), and bichloracetic acid (BCA). The latter are recommended for treating nongenital cutaneous warts.
- Sinecatechins ointment is another treatment option.
Surgery
Surgical interventions commonly are considered for cases with a large number of warts, extensive affected areas, or refractory disease. Physical destruction or excision generally has proven more effective than medical therapy. Primary surgical options include the following:
-
Cryosurgery
-
Electrosurgery (electrodesiccation or loop electrosurgical excision procedure [LEEP])
-
Simple surgical excision using a scalpel, scissors, or curette
Alternative surgical procedures include the following:
-
Carbon dioxide laser ablation
-
Cavitron Ultrasonic Surgical Aspiration (CUSA)
-
Mohs surgery
Vaccines are available for preventing HPV infection, with recommended vaccination schedules established.
Allopathic Treatment for Human papilloma virous
According to that allopathic study, warts might resolve on their own in less than a year (which is not true – said Dr. Qaisar Ahmed), some allopathic doctors may choose to wait for spontaneous resolution instead of undergoing treatment. Available allopathic therapies for anogenital warts may reduce but are unlikely to completely eradicate HPV infectivity or risk of developing cancer.
Allopathic goals
The primary goal of allopathic treatment is to eradicate or reduce symptoms. Allopathic treatment is typically reserved for visible warts only. The general strategy involves removing as many visible lesions as possible until the host immune system can manage viral replication.
Treating subclinical anogenital or mucosal HPV infections in the absence of dysplasia is not recommended, as there is no evidence that treatment eliminates HPV infection or reduces infectivity. Recurrence of warts after allopathic treatment can occur due to activation of latent virus in surrounding healthy skin.
There is not any treatment for HPV in allopathy, although various therapies exist for genital warts, no single modality has demonstrated superiority, and no single allopathic treatment is ideal for all wart types. Factors influencing treatment decisions include lesion size, morphology, number, location, cost, adverse effects, patient preferences, prior treatments, and doctor’s experience.
Common treatments involve direct lesion ablation such as surgical excision, chemical ablation, and cryotherapy. Improper use of these treatments can lead to unnecessary tissue damage. Most patients require multiple treatments over weeks to months. If substantial improvement is not seen after three physician-administered treatments or complete clearance is not achieved after six treatments, a different approach should be considered.
HIV-positive patients or those immunosuppressed may require multiple treatment methods, as their warts often do not respond well to therapy. Recurrence is noted in 20-30% of patients regardless of the chosen therapy, which can be frustrating for both patients and physicians alike.
Pharmacologic Therapy
Both provider-applied treatments and patient-applied treatments are available for HPV disease. All allopathic medications used for treatment are applied topically on cutaneous surfaces. Local skin reactions and pain are common adverse effects. These allopathic medications should not be applied to mucosal surfaces, dysplastic lesions, squamous cell carcinoma (SCC), verrucous carcinoma, or Bowenoid papulosis.
There are two broad categories of allopathic medications effective in treating HPV disease: 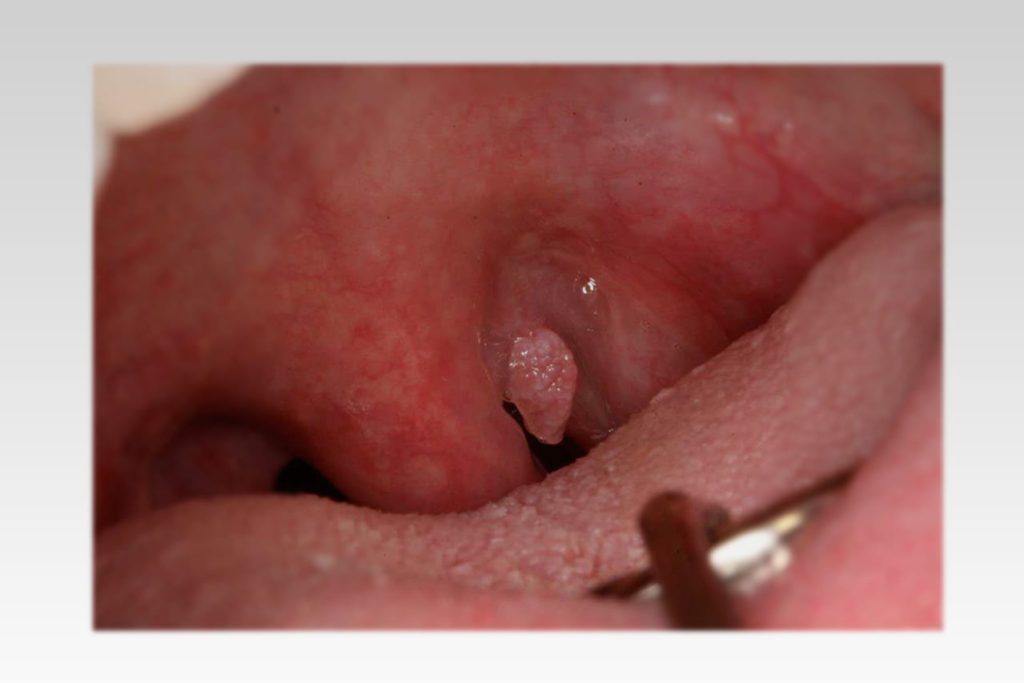
- Cytotoxic agents: These include podofilox, podophyllin, 5-fluorouracil (5-FU), trichloroacetic acid (TCA), and bichloracetic acid (BCA).
- Immune response modifiers: These include imiquimod, sinecatechins and interferon alfa, primarily used for external anogenital warts (condylomata acuminata).
None of these medications have been uniformly effective or shown direct antiviral effects. Keratolytics are the only allopathic agents recommended for nongenital cutaneous warts.
Podofilox:
Podofilox gel or solution is the first-line allopathic treatment choice for external genital warts in nonpregnant patients. It is applied twice daily for 3 consecutive days each week, repeated for up to 4 weeks, and stimulates necrosis of wart tissue. No more than 0.5 g of gel per day should be used limiting the total wart tissue treated to 10 cm2 or less (could be severe side effects).
Podophyllin:
Podophyllin resin, containing podophyllotoxin, is a cytotoxic agent used for physician-applied treatment of external genital warts. It can be applied weekly for up to 6 weeks, but warts visible after 6 treatments may not respond further. Podophyllin must be applied sparingly to avoid toxicity and systemic absorption, with potential side effects including ulceration and neurologic toxicity. It is contraindicated in pregnancy.
5-Fluorouracil (5-FU):
5-FU interferes with DNA and RNA synthesis, causing cell death. Limited data on efficacy exist, with clearance rates reported in 10-50% of cases. It is applied 1-3 times per week for several weeks, with potential side effects including pain and burning. Proper application to prevent pain and ulceration is crucial, as this therapy may not be well-tolerated. A meta-analysis of 6 trials involving 645 women concluded that topical treatment with 5-FU has a therapeutic effect; the data about the side effects, the risks and benefits, and further studies were recommended.
Keratolytics:
TCA and BCA are potent keratolytic agents used for all types of cutaneous warts, while salicylic acid is milder and used primarily for nongenital warts.
In an 80-90% concentration TCA is used for treating vulvar or vaginal condyloma in pregnant women. TCA should be applied to the condyloma after pretreatment of the surrounding normal skin with petroleum jelly. As the acid dries, a white frosting develops, which should be powdered with sodium bicarbonate to neutralize any unreacted acid.
Effective treatment usually requires weekly applications for 4-6 weeks. The principal side effect is pain and burning if the TCA comes in contact with normal skin. Although TCA is caustic, it causes less local irritation and systemic toxicity than other agents in the same class. However, the response is often incomplete, and recurrence is common.
Imiquimod:
Imiquimod stimulates cytokine production (including interferon alfa) but lacks direct antiviral activity. It is effective for external genital warts, with up to 50% clearance in clinical trials. Two formulations are available, Aldara (5 percent imiquimod) and Zyclara (3.75 percent imiquimod). Aldara is applied on three alternate days per week for up to 16 weeks. Zyclara is applied daily for up to 8 weeks. It should be washed off after 8 hours. Recurrence rates at 6 months range from 19-23%. Common side effects include erythema, itching, and burning.
Sinecatechins:
Sinecatechins ointment, applied 3 times daily for up to 16 weeks, has demonstrated good clearance of external genital warts in clinical trials, with a recurrence rate as low as 5%. Side effects include erythema, pruritus, and pain.
Interferon Alfa:
Interferon alfa is a naturally occurring cytokine produced either through recombinant DNA technology or from pooled human leukocytes. It has potent immunomodulatory and direct antiviral effects. Local injection of interferon appears to be more effective than systemic injection.
Interferon alfa is used for the intralesional treatment of external anogenital warts and condyloma acuminatum. Intralesional injection of 0.5 to 1.5 million international units per lesion is administered two to three times per week for up to three weeks. For large warts, it may be injected at several points around the periphery in a total dose of 250,000 IU per wart. The course of therapy can be repeated 12 to 16 weeks from the initial treatment.
Patients with 6-10 condylomata may receive a second course of treatment using the same dosage schedule to treat up to five additional condylomata per course. Patients with more than ten condylomata may receive additional sequences, depending on the number of condylomata present.
Recurrence rates are 21%, side effects included flu-like symptoms, fatigue, and pain. Interferon is contraindicated in pregnancy.
Complications with allopathic treatment
Overall, complications of wart treatment are generally confined to the treatment site and include scarring and, in the case of genital warts, vulvodynia or hyperesthesia.
Each allopathic therapeutic modality carries its own unique set of risks. Expected effects of cryosurgery include pain, edema, vesicles, bullae, weeping, and some necrosis. There is a small risk of infection, bleeding, abnormal scarring, pigment alteration, paresthesia, and alopecia with cryosurgery.
Similarly, laser therapy for genital warts may result in pigment alteration, abnormal scarring, and infection. Special care must be taken to prevent respiratory infection from the laser plume generated by vaporization of virally infected tissue.
Plantar warts can disrupt ambulation due to their location. Laryngeal papillomas may interfere with breathing or speaking. Genital warts occasionally lead to issues such as urethral obstruction. Condylomata acuminata can grow extremely large, resulting in tissue breakdown or secondary infection. In the context of immune deficiency, such as HIV infection, HPV-induced wart growth can be exacerbated, significantly worsening associated anatomical problems (see the image below).

Serious complication
Patients who develop condylomata acuminata typically are exposed to low-risk HPV types such as HPV-6 and HPV-11. These HPV infections are associated with mild dysplasia that often resolves spontaneously. Many patients with mild dysplasia of the vulva, vagina, or cervix experience regression of these lesions without intervention. In contrast, patients exposed to high-risk HPV types, such as HPV-16 or HPV-18, usually do not develop condylomata. Instead, they are at risk for high-grade dysplasia or anogenital carcinoma.
Homeopathic treatment for Human papilloma virous
The goal of Homeopathic treatment is to remove warts and alleviate any present symptoms and cause(s). The appearance of warts can cause significant psychosocial distress, and their removal can address cosmetic concerns. Homeopathic medicines teats all types of HPV and there underlying causes. Due to their anti-viral activities, there are no recurrence in all cases and in any stage.
What is the Homeopathic treatment for warts/HPV?
The primary goal of Homeopathic treatment is to eradicate/treat the disease itself along with the root cause(s) and reduce discomfort and symptoms. Treatment is typically reserved for all visible and nonvisible warts. Recurrence of warts after Homeopathic treatment is almost zero percent (0%).
How can I remove warts?
Here are some Homeopathic medicines for HPV and condylomas:
Natrium Sulphuricum
Tendency to warts. Itching while undressing. Jaundiced, watery blisters. Sycotic excrescences; wart-like red lumps all over body. Fingers and toes affected. Granular lids. Photophobia. Slimy, thick, tenacious, white mucus. Bitter taste, blisters on palate. Swelling of axillary glands. Inflammation around root of nails. Burning in soles; edema of feet; itching between toes.
Mezereum
Post-nasal adenoids. Herpes zoster. Skin.-Sensitiveness to touch.-General desquamation of skin of body; usual liver spots on chest and arms become dark and desquamate.-Red rash, itching violently; < in bed, from touch; burning and change of place after scratching.-Cutaneous ulcers form over bony protuberances.-Ulcers with thick, whitish, yellow scabs, under which thick, yellow pus collects.-Skin covered with elevated white scabs. Itching
Thuja Occidentalis
Acts on skin, blood, gastro-intestinal tract, kidneys, and brain. Its relation to the production of pathological vegetations condylomas, warty excrescences, spongy tumors. Bleeding fungus growths. formation of wart-like excrescences upon mucous and cutaneous surfaces-fig-warts and condylomas. Suppressed gonorrhea, salpingitis. Ill-effects/side effects of vaccination. Chronic otitis; discharge purulent. Creaking when swallowing. Polyps. Tip of tongue very painful. White blisters on side close to root, painfully sore.
Polyps – tubercles, warts epithelioma, naevi, carbuncles; ulcers. Freckles and blotches. Perspiration sweetish, and strong. Dry skin, with brown spots. Zona; herpetic eruptions. Tearing pains in glands. Glandular enlargement. Nails crippled; brittle and soft. Eruptions only on covered parts; worse after scratching, very sensitive to touch. Coldness of one side. Sarcoma; polyps, warts. Brown spots on hands and arms. 
Rhus Toxicodendrone
Rhus affects fibrous tissue. Orbital cellulitis. Pustular inflammations. Skin red, swollen; itching intense. Vesicles, herpes; urticaria; pemphigus; erysipelas; vesicular suppurative forms. Glands swollen. Cellulitis. Burning eczematous eruptions with tendency to scale formation. Vesicular erysipelas where the vesicles are large. Exanthema. Black pustules. Herpes, sometimes alternately with asthmatic sufferings and dysenteric looseness. Warts, especially on hands and fingers; large jagged, often pedunculated, exuding moisture and bleeding readily. Rhagades on hands. arms. . Tingling or shooting or else burning smarting in ulcers. Chilblains. Corns on feet, with burning sensation, and pain as of excoriation.
Graphite
A best anti psoric (antiviral). Skin: Rough, hard, persistent dryness of portions of skin unaffected by eczema. Early stage of keloid and fibroma. Pimples and acne. Eruptions, oozing out a sticky exudation. Rawness in bends of limbs, groins, neck, behind ears. Unhealthy skin; every little injury suppurates. Ulcers discharging a glutinous fluid, thin and sticky. Swelling and induration of glands. Gouty nodosities. Cracks in nipples, mouth, between toes, anus. Phlegmonous erysipelas of face; burning and stinging pain. Swelling of feet. Wens.
Hydrastis Canadensis
Eruption like variola. Lupus; ulcers, cancerous formations. Moles. Warts. General tendency to profuse perspiration and unhealthy skin.
Calcar Carbonica
Skin unhealthy; readily ulcerating; flaccid. Small wounds do not heal readily. Glands swollen. Nettle rash. Warts on face and hands. Petechial eruptions. Chilblains. Boils.
Silica Tera
Felons, abscesses, boils, old fistulous ulcers. Delicate, pale, waxy. Cracks at end of fingers. Painless swelling of glands. Rose-colored blotches. Scars suddenly become painful. Pus offensive. Promotes expulsion of foreign bodies from tissues. Every little injury suppurates. Long lasting suppuration and fistulous tracts. Dry fingertips. Eruptions itch only in daytime and evening. Crippled nails. Indurated tumors. Abscesses of joints. After impure vaccination. Bursa. Lepra, nodes, and coppery spots. Keloid growths. 
Sabina
Fig-warts, with intolerable itching and burning. Exuberant granulations. Warts. Black pores in skin.
Antimunium Tartaricum
Pustular eruption, leaving a bluish-red mark. Smallpox. Warts. Itching in the skin. Itching pimples, and miliary eruption. Eruptions like scabies.
Anagallis Arvensis
Marked action on skin. Itching; dry, bran-like eruption, especially on hands and fingers. Palms especially affected. Vesicles in groups. Ulcers and swellings on joints. Favors expulsion of splinters. An old medicine for hydrophobia and dropsy. Possesses power of softening flesh and destroying warts.
Dulcamara
Adenitis. Pruritus, always worse in cold, wet weather. Herpes zoster, pemphigus. Swelling and indurated glands from cold. Vesicular eruptions. Sensitive bleeding ulcers. Little boils. Red spots, urticaria, brought on by exposure, or sour stomach. Humid eruptions on face, genitals, hands, etc. Warts, large, smooth, on face and palmar surface of hands. Anasarca. Thick, brown-yellow crusts, bleeding when scratched.
Causticum
Soreness in folds of skin, back of ears, between thighs. Warts large, jagged, bleeding easily, on tips of fingers and nose. Old burns that do not get well, and ill effects from burns. Pains of burns. Cicatrices freshen up; old injuries reopen. Skin prone to intertrigo during dentition.
Petroleum
Itching at night. Chilblains, moist, itch and burn. Bedsores. Skin dry, constricted, very sensitive, rough and cracked, leathery. Herpes. Slightest scratch makes skin suppurate. Intertrigo; psoriasis of hands. Thick, greenish crusts, burning and itching; redness, raw; cracks bleed easily. Eczema.
Nitric Acidum

Warts, large jagged; bleed on washing. Ulcers bleed easily, sensitive; splinter-like pains; zigzag, irregular edges; base looks like raw flesh. Exuberant granulations. Black pores on face, papules.
Kalium Arsenicosum
The Kali ars patient tends towards malignancy, and inveterate skin diseases. Restless, nervous and anemic. Intolerable itching, worse undressing. Dry, scaly, wilted. Acne; pustules worse during menses. Chronic eczema; itching worse from warmth, walking, undressing. Psoriasis, lichen. Phagedenic ulcers. Fissures in bends of arms and knees. Gouty nodosities; worse, change of weather. Skin cancer, where suddenly an alarming malignancy without any external signs sets in. Numerous small nodules under skin. Cauliflower like warts.
Kalium Muriaticum
Acne, erythema, and eczema, with vesicles containing thick, white contents. Dry, flour-like scales on the skin. Bursitis. Inflammatory states, fibrinous exudations, and glandular swellings.
Heper Sulphuricum
Abscesses; suppurating glands are very sensitive. Papules prone to suppurate and extend. Acne in youth. Suppurate with prickly pain. Easily bleed. Angio-neurotic edema. Unhealthy skin; every little injury suppurates. Chapped skin, with deep cracks on hands and feet. Ulcers, with bloody suppuration, smelling like old cheese. Ulcers very sensitive to contact, burning, stinging, easily bleeding. Sweats day and night without relief. “Cold-sores” very sensitive. Cannot bear to be uncovered; wants to be wrapped up warmly. Sticking or pricking in afflicted parts. Putrid ulcers, surrounded by little pimples. Great sensitiveness to slightest touch. Chronic and recurring urticaria. Smallpox. Herpes circinate. Constant offensive exhalation from the body.
Sepia
Herpes circinate in isolated spots. Itching; not relieved by scratching; worse in bends of elbows and knees. Chloasma; herpetic eruption on lips, about mouth and nose. Ringworm-like eruption every spring. Urticaria on going in open air; better in warm room. Hyperidrosis and bromhidrosis. Sweat on feet, worse on toes, intolerable odor. Lentigo in young women. Ichthyosis with offensive odor of skin.
Sarsaparilla

Emaciated, shriveled, lies in folds, dry, flabby. Herpetic eruptions; ulcers. Rash from exposure to open air; dry, itching; comes on in spring; becomes crusty. Rhagades; skin cracked on hands and feet. Skin hard, indurated. Summer cutaneous affections.
Natrum Muriaticum
Greasy, oily, especially on hairy parts. Dry eruptions, especially on margin of hairy scalp and bends of joints. Fever blisters. Urticaria; itch and burn. Crusty eruptions in bends of limbs, margin of scalp, behind ears. Warts on palms of hands. Eczema; raw, red, and inflamed; worse, eating salt, at seashore. Affects hair follicles. Alopecia. Hives, itching after exertion. Greasy skin.
Kreosotum
Itching, worse towards evening. Burning in soles. Senile gangrene. Small wounds bleed freely. Pustules and herpes. Ecchymosis; dorsal surface of fingers and hands eczematous.
Medorrhinum
Skin yellow. Intense and incessant itching; worse night and when thinking of it. Fiery red rash about anus in babies. Copper-colored spots. Favus. Tumors and abnormal growth.
Variolinum
Exanthema of sharp, pointed pimples, usually small, seldom large and suppurating, dry, resting on small red areolae, frequently interspersed with spots of red color, sometimes severe itching. Petechial eruptions. Shingles.
Sulphur

Skin dry, scaly, unhealthy; every little injury suppurates. Freckles. Itching, burning; worse scratching and washing. Pimply eruption, pustules, rhagades, hangnails. Excoriation, especially in folds. Feeling of a band around bones. Skin affections after local medication. Pruritus, especially from warmth, in evening, often recurs in spring and in damp weather.
Tellurium Metallicum
Itching of hands and feet. Herpetic spots; ringworm. Ring-shape lesions, offensive odors from affected parts. Barber’s itch. Stinging in skin. Fetid exhalations. Offensive foot-sweat. Eczema, offensive discharges. Circular patches of eczema. Otorrhea – itching, swelling, throbbing in meatus. Deafness.
Antimonium Crudum
Eczema with gastric derangements. Pimples, vesicles, and pustules. Sensitive to cold bathing. Thick, hard, honey-colored scabs. Urticaria; measles-like eruption. Itching when warm in bed. Dry skin. Warts. Dry gangrene. Scaly, pustular eruption with burning and itching, worse at night.
Carcinosin
Cutaneous warts are hyperkeratotic protrusions over the skin caused by human papilloma
virus (HPV). Typical warts, tender when growing beneath the nail plate and fissured. Periungual warts common around the nails, especially beneath the nail and nail folds and can significantly disturb nail growth. Plane warts – flat, marginally raised and generally skin-colored or greyish yellow, may be pigmented. Warts may be flat, rough and painful papulonodular epidermal lesions over different body parts.
Prognosis
What is the outlook for people with warts?
HPV infection primarily involves the basal epithelial cells, leading to common recurrences and regressions. The prognosis generally is good, and most cases of genital warts are treatable. However, patients who do not develop immunity to HPV may face potentially serious sequelae.
Genital warts can spontaneously regress, remain unchanged, or increase in size. Treating these lesions does not impact the development of cervical cancer. Approximately two-thirds of patients with nongenital cutaneous warts experience spontaneous regression within 2 years, although new warts may appear.
HPV infection of the vulva can result in vulvar intraepithelial neoplasia (dysplasia) or squamous cell carcinoma of the vulva. Most research indicates a strong association between HPV infection and the development of cervical dysplasia and cervical carcinoma. HPV accounts for more than 99% of the attributable risk for cervical dysplasia. Vaginal dysplasia and vaginal cancer also are linked to HPV exposure.
Histology
Histologic evidence of HPV infection on a cervical Pap smear resembles mild dysplasia. This subclinical disease often regresses spontaneously.
There is a direct correlation between anogenital HPV infection and measures of sexual activity, such as the age of first intercourse and the lifetime number of sexual partners. Women with a history of high-grade squamous intraepithelial lesion (HGSIL) of the cervix or invasive squamous cell carcinoma (SCC) of the cervix are at increased risk of developing invasive cancer in other anogenital mucosal tissues, particularly vaginal and anal carcinoma. In these patients, the relative risk for vaginal carcinoma is 5.6, and the risk of anal carcinoma is 4.
Women who are immunocompromised due to immunosuppressive drug therapy or HIV infection are at higher risk for persistent HPV disease. These women are more likely to develop dysplasia or cancer of the vulva, vagina, or cervix.
Anal cancer
Anal cancer is strongly associated with male homosexuality and specific male practices, such as engaging in receptive anal intercourse. The relative risk is 33. However, the overall disease prevalence is higher in women than in men, with a female-to-male ratio of 1.5:1.
Men infected with HPV are at risk for genital warts. The 24-month risk varies from 57.9% in men infected with HPV type 6 or type 11 to 2% in men infected with other HPV types.
Immunosuppressed patients, particularly those with cutaneous malignant lesions, have a much higher incidence of EV-HPV infection than the general population. These lesions can undergo malignant transformation. About 10% of patients with EV originate from consanguineous marriages, suggesting an autosomal recessive mode of inheritance.
Most patients with EV experience disease progression in the third or fourth decades of life. Malignant transformation usually arises from actinic keratoses, especially in patients exposed to irradiation. Patients who avoid x-rays and sun exposure generally maintain satisfactory health.
As many as 20% of patients with genital warts have other sexually transmitted diseases concurrently. In an Australian sexual health clinic, 5% of patients with genital warts also were found to have chlamydia and/or gonorrhea.
P. S: This article is only for doctors and students having good knowledge about Homeopathy and allopathy.

For proper consultation and treatment, please visit our clinic.
 Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Senior research officer at Dnepropetrovsk state medical academy Ukraine.
Location: Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Find more about Dr Sayed Qaisar Ahmed at:
https://www.youtube.com/Dr Qaisar Ahmed
But wanna remark on few general things, The website style and design is perfect, the subject matter is real excellent. “Taxation WITH representation ain’t so hot either.” by Gerald Barzan.