
Chronic and Acute Bronchitis is a term that describes inflammation of the bronchial tubes (bronchi and the smaller branches termed bronchioles) that results in excessive secretions of mucus into the tubes, leading to tissue swelling that can narrow or close off bronchial tubes. Bronchial tubes extend from the trachea and terminate at the alveoli in the lungs. The bronchial system resembles an inverted tree and is sometimes termed the “bronchial tree”.
There are two major types of bronchitis, acute and chronic. Chronic bronchitis differs from acute bronchitis in several ways, for example, pathology, progression of disease, major causes, treatments, and prognosis. Recurrent incidences of acute bronchitis are the first steps that can lead to developing chronic bronchitis.
Chronic bronchitis is defined as a cough that occurs every day with sputum production that lasts for at least 3 months, two years in a row. This definition was developed to help select uniform patient populations for research purposes, for example, to study medication therapies for the treatment of chronic bronchitis.
Many of the bronchi develop chronic inflammation with swelling and excess mucus production. The inflammation causes a change in the lining cells of the airways to varying degrees. Many cells that line the airway lose the function of their cilia (hair-like appendages that are capable of beating rapidly), and eventually, the ciliated cells are lost.
Cilia perform the function of moving particles and fluid (usually mucus) over the lining surface in such structures as the trachea, bronchial tubes, and nasal cavities to keep these hollow structures clear of particles and fluids. These ciliated cells that help in the clearance of secretions are often replaced by so-called goblet cells. This group of cells secretes mucus into the airway. The warm moist environment of the airway along with the nutrients in the mucus is an excellent medium for growing bacteria. The mucus often becomes infected and discolored from the bacterial overgrowth and the body’s inflammatory response to it. The inflammation, swelling, and mucus frequently and significantly inhibit the airflow to and from the lung alveoli by narrowing and partially obstructing the bronchi and bronchioles.
The muscles that surround some of the airways can be stimulated by this airway irritation. This muscular spasm also known as bronchospasm can result in further airway narrowing. With long-standing inflammation, as can be seen in chronic bronchitis, this muscular spasm and inflammation result in a fixed, nonreversible narrowing of the airway, and the condition is termed chronic obstructive pulmonary disease (COPD).
Chronic coughing develops as the body attempts to open and clear the bronchial airways of particles and mucus or as an overreaction to ongoing inflammation. Chronic bronchitis can be a progressive disease; symptoms increase over time. Some NIH investigators consider chronic bronchitis a type of COPD.
COPD also includes the entities of emphysema, chronic bronchitis, and chronic asthma. These conditions are not always separable, and patients often have components of each. In the case of chronic bronchitis, the fixed airway obstruction, airway inflammation, and retained secretions can result in a mismatch of blood flow and airflow in the lungs. This can impair oxygenation of the blood and in result the removal of the waste product, carbon dioxide.
Symptoms of chronic bronchitis
The major signs and symptoms of chronic bronchitis are:
- Cough and sputum production are the most common symptoms. They usually last for at least 3 months and occur daily. The intensity of coughing and the amount and frequency of sputum production vary from patient to patient. Sputum may be clear, yellowish, greenish, or occasionally, blood tinged. Since cigarette smoke is the most common cause for chronic bronchitis, it should not be surprising that the most common presentation is so called smoker’s cough. This is characterized by a cough that tends to be worse upon arising and is often productive of discolored mucus in the early part of the day. As the day progresses, less mucus is produced.
- Shortness of breath (dyspnea) gradually increases with the severity of the disease. Usually, people with chronic bronchitis get short of breath with activity and begin coughing; dyspnea at rest usually signals that COPD or emphysema has developed.
- Wheezing (a coarse whistling sound produced when airways are partially obstructed) often occurs.
Other signs and symptoms that may accompany chronic bronchitis include
- fatigue,
- sore throat,
- muscle aches,
- nasal congestion, and
- headaches.
Exacerbation of chronic bronchitis occurs when symptoms worsen or become more frequent. Signs and symptoms of exacerbation of chronic bronchitis include:
- Severe coughing that causes chest discomfort or chest pain.
- Cyanosis (bluish/grayish skin coloration) may develop in people with advanced COPD.
- Fever may indicate a secondary viral or bacterial lung infection.
Causes of chronic bronchitis
There are many causes of chronic bronchitis, but the main cause is tobacco smoke.
- Many other inhaled irritants (for example, smog, industrial pollutants, and solvents) can also result in chronic bronchitis.
- Viral and bacterial infections that result in acute bronchitis may lead to chronic bronchitis if people have repeated bouts with infectious agents.
- Also, underlying disease processes (for example, asthma, cystic fibrosis, immunodeficiency, congestive heart failure, familial genetic predisposition to bronchitis, and congenital or acquired dilation of the bronchioles, known as bronchiectasis) may cause chronic bronchitis to develop, but these are infrequent causes compared to tobacco smoking.
There are others risk factor, such as:
- repeated exposure to pollutants (especially airborne materials such as ammonia, sulfur dioxide, chlorine, bromine, hydrogen sulfide).
- dust.
- repeated bouts of acute bronchitis or pneumonia.
- gastric reflux (by inhalation of gastric contents).
Diagnose Chronic and Acute Bronchitis 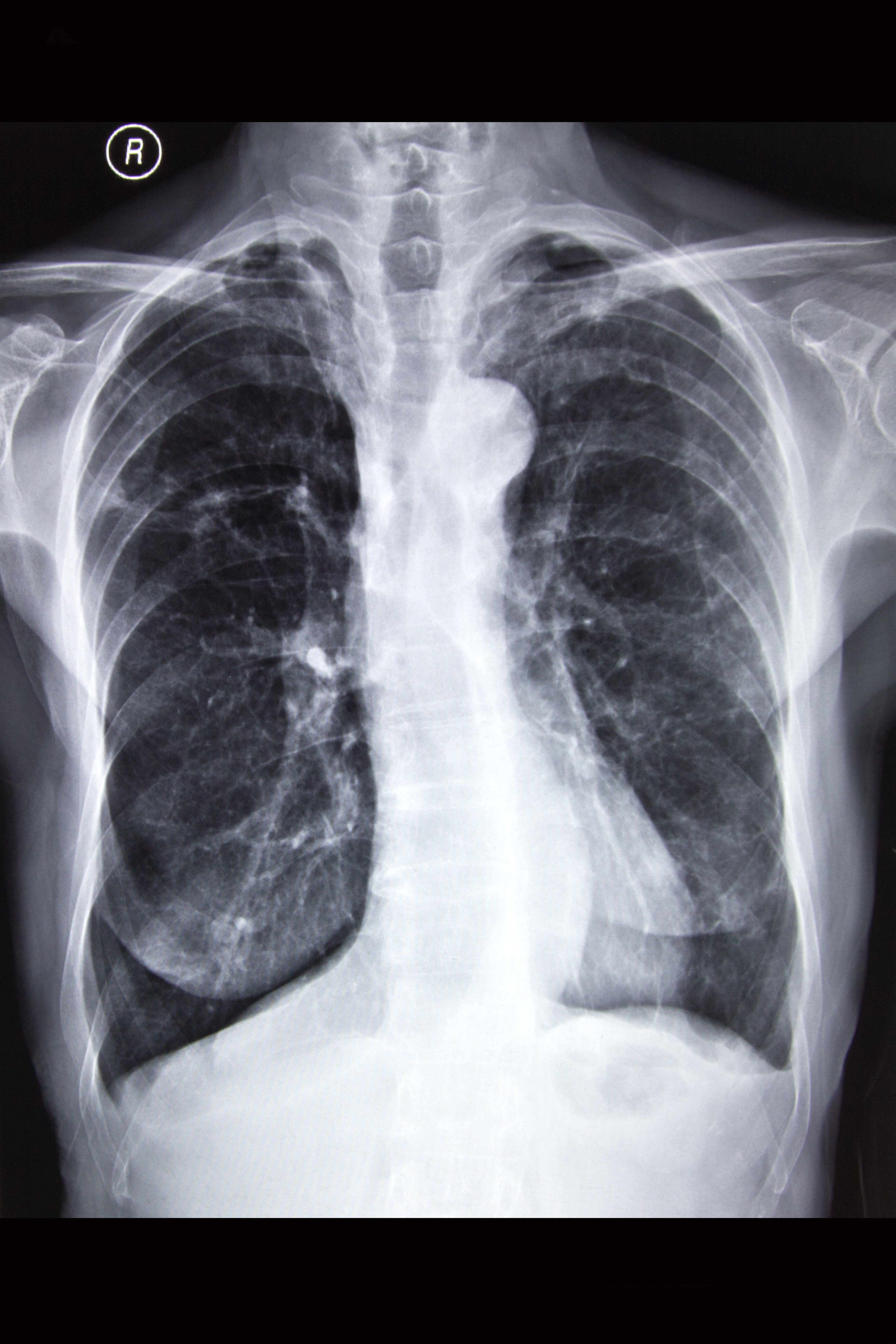
Diagnose of Chronic and Acute Bronchitis based on a patient’s medical history, physical exam, and diagnostic tests. A history of a daily productive (sputum production) cough that lasts at least 3 months, especially if has occurred two years in a row, fits the criteria for a clinical diagnosis of chronic bronchitis. The physical examination often allows health-care professionals to hear wheezes and a prolongation of the exhalation of breathing, which are signs of airflow obstruction.
A chest X-ray is often performed to help rule out other lung problems (for example, pneumonia, bronchial obstructions). Additional tests such as a complete blood count (CBC), arterial blood gas measurements, CT scan of the chest, and pulmonary function tests are often done to characterize the structure and function of the lungs and to help exclude other conditions (for example, lung cancer, tuberculosis, lung infections).
Treatment for Chronic and Acute Bronchitis
Patient should be encouraged in every way to stop and ease smoking, as continuation will only cause further lung damage. Similarly, blocking or removing other underlying causes of repeated bronchial irritation (for example, exposure to chemical fumes) is a treatment goal.
In Allopathy two major classes of medications are used to treat chronic bronchitis, bronchodilators, and steroids.
- Bronchodilators, metaproterenol, formoterol work by relaxing the smooth muscles that encircle the bronchi, which allows the inner airways to expand. Anticholinergic drugs also can act as bronchodilators, including tiotropium and ipratropium.
- Steroids reduce the inflammatory reaction and thus decrease the bronchial swelling and secretions that in turn allows better airflow because of reduced airway obstruction. Often inhaled steroids are administered since they have fewer side effects than systemic (oral) steroids. Combination therapy with both steroids and bronchodilators is often utilized.
Allopathic treatment for Chronic and Acute Bronchitis
PDE4 inhibitors are a class of anti-inflammatory agents for certain exacerbations of COPD. They are primarily for exacerbations that involve excessive bronchitis and mucus production. There is currently only one agent available called roflumilast.
Antibiotics: Occasionally, antibiotics are used to treat chronic bronchitis exacerbations caused by bacterial infections. Broad-spectrum antibiotics are often the choice. Examples include:
- Fluoroquinolones (levofloxacin).
- Macrolides (clarithromycin, azithromycin).
- Sulfonamides (sulfamethoxazole and trimethoprim).
- Tetracyclines (doxycycline).
If a culture is obtained, directed therapy at the specific offending organism is always best.
Over the counter (OTC) cough suppressants such as dextromethorphan may be helpful in reducing cough symptoms. OTC preparations with guaifenesin may make patients feel more comfortable but there is no scientific evidence that it helps mucus to become less viscous.
Homeopathic Treatment of Chronic and Acute Bronchitis
Ipecacuanha
Dyspnea, constant constriction in chest. Asthma. Yearly attacks of difficult shortness of breathing. Continued sneezing; coryza; wheezing cough. Cough incessant and violent, with every breath. Chest seems full of phlegm but does not yield to coughing. Bubbling rales. Suffocative cough: patient becomes stiff, and blue in the face. Whooping-cough, with nosebleed, and from mouth. Bleeding from lungs, with nausea; feeling of constriction; rattling cough. Croup. Hemoptysis from slightest exertion. Hoarseness, especially at end of a cold. Complete aphonia.
Stannum Metallicum
Chief action is centered upon the nervous system and respiratory organs. Debility, especially the debility of chronic bronchial and pulmonary conditions. Profuse muco-purulent discharges upon tuberculosis basis. Talking causes a very weak feeling in the throat and chest. Pains that come and go gradually. Paralytic weakness; spasms; paralysis.
Headache – aching in temples and forehead. Obstinate acute coryza and influenza with cough. Drawing pains in malar bones and orbits. Much adhesive mucus in throat, difficult to detach; efforts to detach cause nausea. Throat dry and stings. Hoarse; mucus expelled by forcible cough. Violent, dry cough in evening until midnight. Cough excited by laughing, singing, talking; worse lying on right side. During day, with copious green, sweetish, expectoration. Chest feels sore. Chest feels weak; can hardly talk. Influenzas cough from noon to midnight with scanty expectoration. Respiration short, oppressive; stitches in left side when breathing and lying on same side. Phthisis mucosa. Hectic fever. Sleeps with one leg drawn up, the other stretched out.
Smell of cooking causes vomiting. Bitter taste. Pain better pressure, but sore to touch. Sensation of emptiness in stomach.
Drosera Rotundfolia
Affects markedly the respiratory organs and is the principal remedy for whooping-cough. Drosera can break down resistance to tubercle. Phthisis pulmonal; vomiting of food from coughing with gastric irritation and profuse expectoration. Spasmodic, dry irritative cough, whooping cough. yellow expectoration, with bleeding from nose and mouth, laryngitis. Rough, scraping sensation deep in the faucet and soft palate.
Antimuonium Tartaricum 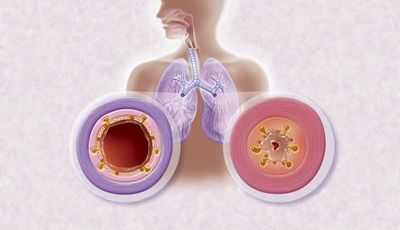
Rattling of mucus with little expectoration with drowsiness, debility and sweat, trembling of whole body, great prostration and faintness. Hoarseness. Rattling of mucus, but hard to expectorate. Burning sensation in chest. Cough excited by eating, with pain in chest and larynx. Edema and impending paralysis of lungs.
Coldness, trembling, and chilliness. Intense heat. Copious perspiration. Cold, clammy sweat, with great faintness. Intermittent fever with lethargic condition.
All symptoms worse, in evening; from lying down at night; from warmth; in damp cold weather; from all sour things and milk. Better, from sitting erect; from eructation and expectoration.
Pulsatilla Pratensis
Capricious hoarseness; comes and goes. Chronic and acute bronchitis. Dry cough in evening and at night; must sit up in bed to get relief; and loose cough in the morning, with copious mucous expectoration. Pressure upon the chest and soreness. Great soreness of epigastrium. Urine emitted with cough. Pain as from ulcer in middle of chest. Expectoration bland, thick, bitter, greenish. Short breath, anxiety, and palpitation when lying on left side. Smothering sensation on lying down.
Ammonium Carbonicum
Hoarseness. Cough every morning. Emphysema. Burning in chest. Asthenic Pneumonia. Rattling pulmonal sounds. Slimy sputum and specks of blood. Pulmonary edema. Chronic and acute bronchitis. Tearing in joints relieved by heat of bed; inclination to stretch limbs. Hands cold and blue; distended veins. Fingers swell when arm is hanging down. Extremities heaviness. Chronic gout. Nodosoties. Facial paralysis. Panaritium, deep-seated periosteal pain. Cramps in calves and soles. Big toe painful and swollen. Felons in the beginning. Heel painful on standing. Tearing in ankle and bones of feet. Bronchitis of late stages (3rd). Calculi.
All symptoms worse in warm, especially in morning (warm room/bed).
Conium Maculate
Dry hacking cough, almost continuous; worse, evening and at night, when lying down, talking or laughing, and during pregnancy. Expectoration only after long coughing. Chronic and acute bronchitis.
The patient has a cough at night on lying down. They are restless at night and tend to sit up many times due to coughing spells. A tickling sensation in the throat pit may be prominently present. A few individuals may complain of an unusually dry spot in the larynx. In some cases, a headache on coughing may arise.
Ipecacuanha
The chief action is on the ramifications of the pneumogastric nerve, producing spasmodic irritation in chest and stomach. Dyspnea; constant constriction in chest. Asthma. Yearly attacks of difficult shortness of breathing. Continued sneezing; coryza; wheezing cough. Chronic and acute bronchitis. Cough incessant and violent, with every breath. Chest seems full of phlegm but does not yield to coughing. Bubbling rales. Suffocative cough: patient becomes stiff, and blue in the face. Whooping-cough, with nosebleed, and from mouth. Bleeding from lungs, with nausea; feeling of constriction; rattling cough. Croup. Hemoptysis from slightest exertion. Hoarseness, especially at end of a cold. Complete aphonia.
Spongia Tosta
A remedy especially marked in the symptoms of the respiratory organs, cough, croup, thyroid gland swollen. stitches and dryness in throat, burning stinging and sore throat etc. Tickling causes cough. Clears throat constantly. Laryngeal phthisis. Goiter.
Great dryness of all air-passages. Hoarseness: larynx dry, burns, constricted. Cough, dry, barking, croupy; larynx sensitive to touch. Croup; worse, during inspiration and before midnight. Respiration short, panting, difficult; feeling of a plug-in larynx. Chronic and acute bronchitis. Cough abates after eating or drinking, especially warm drinks. Wheezing asthmatic cough, worse cold air and lying, head low and in warm, with profuse expectoration and suffocation. Oppression and heat of chest.
Swelling and induration of glands; also, exophthalmic; cervical glands swollen with tensive pain on turning head, painful on pressure; Goiter. Itching; measles
Corallium Rubrum
Whooping and spasmodic coughs, especially when the attack comes on with a very rapid cough, and the attacks follow so closely as to almost run into each other. Often preceded by sensation of smothering, followed by exhaustion. Profuse, nasal catarrh. Cough that results from PND (postnasal dripping). Hawking of profuse mucus. Throat very sensitive, especially to air. Chronic and acute bronchitis.
The cough appears in quick, short attacks that follow each other in quick succession, hysterical cough. Dry, spasmodic, suffocative cough; very rapid cough, short, barking, whooping-cough. Extreme exhaustion is felt along with the cough. A vital symptom that attends the above symptoms are extremely sensitive air passages to air (inhaled air feels cold).
Millifolium
Millifolium is and antiviral medicine. Cough with bloody sputa or in any lung disease with accompanying cough. Chronic and acute bronchitis. Shortness of breath, difficulty in breathing, oppression of chest. Hemoptysis after injury or following violent exertion.
Natrum Muriaticum 
Cough from a tickling in the pit of stomach, accompanied by stitches in liver and spurting of urine. Stitches all over chest. Chronic and acute bronchitis. Cough, with bursting pain in head. Shortness of breath. Whooping-cough with flow of tears with cough and with salty sputum.
Kali Sulph
Rattling of mucus in chest. Post-grippe cough, especially in children. Bronchial asthma, with yellow expectoration. Chronic and acute bronchitis. Cough; worse in evening and in hot atmosphere. Croupy hoarseness.
Pulsatilla Nigricans
Capricious hoarseness. Dry cough in evening and at night; must sit up in bed to get relief; and loose cough in the morning, with copious mucous expectoration. Expectoration bland, thick, bitter, greenish. Short breath, anxiety, and palpitation when lying on left side. Chronic and acute bronchitis.
Heper Sulph
Cough troublesome when walking. Chronic and acute bronchitis. Dry, hoarse cough. Cough excited whenever any part of the body gets cold or uncovered, or from eating anything cold. Croup with loose, rattling cough; worse in morning. Choking cough. Rattling, croaking cough; suffocative attacks; has to rise up and bend head backwards. Anxious, wheezing, moist breathing, asthma worse in dry cold air.
Phosphorus
Cough from tickling in throat; worse, cold air, reading, laughing, talking, from going from warm room into cold air. Sweetish taste while coughing. Hard, dry, tight, racking cough. Congestion of lungs. Burning pains, frothy or blood-stained sputum. The phlegm may be salty or sweet to taste. Strong odors may trigger a cough. Pneumonia, with oppression. Chronic and acute bronchitis.
Arsenic Album
Asthma worse midnight. Burning in chest. Suffocative catarrh. Cough worse after midnight; worse lying on back. Expectoration scanty, frothy. Darting pain through upper third of right lung. Wheezing respiration. Hemoptysis with pain between shoulders; burning heat all over. Cough dry. Chronic and acute bronchitis.
Throat: Swollen, edematous, constricted, burning, unable to swallow. Diphtheritic membrane looks dry and wrinkled.
Bryonia Alba
Soreness in larynx and trachea. Hoarseness; worse in open air. Dry, hacking cough from irritation in upper trachea. Cough, dry, at night; must sit up; worse after eating or drinking, with vomiting, with stitches in chest, and expectoration of rust-colored sputa. Chronic and acute bronchitis. Frequent desire to take a long breath; must expand lungs. Difficult, quick respiration; worse every movement; caused by stitches in chest. Cough, with feeling as if chest would fly to pieces; presses his head on sternum; must support chest. Croupous and pleuro-pneumonia. Expectoration brick shade, tough, and falls like lumps of jelly. Tough mucus in trachea, loosened only with much hawking. Coming into warm room excites cough. Heaviness beneath the sternum extending towards the right shoulder. Cough worse by going into warm room.
Throat: Dryness, sticking on swallowing, scraped and constricted. Tough mucus in larynx and trachea, loosened only after much hawking, worse coming into warm room.
Sambucus Nigra
Hoarseness with tenacious mucus in larynx. Paroxysmal, suffocative cough, coming on about midnight, with crying and dyspnea. Spasmodic croup. Dry coryza. Sniffles of infants; nose dry and obstructed. Loose choking cough. Chronic and acute bronchitis. Patient awakes suddenly, nearly suffocating, sits up, turns blue. Cannot expire. Millar’s asthma.
Mephitis Putorius
Sudden contraction of glottis, when drinking or talking. Food goes down wrong way. False croup; cannot exhale. Chronic and acute bronchitis. Spasmodic and whooping-cough. Few paroxysms in daytime, but many at night; with vomiting after eating. Asthma, as if inhaling Sulphur; cough from talking; hollow, deep, with rawness, hoarseness, and pains through chest. Violent spasmodic cough; worse at night.
Senega 
Hoarseness. Hurts to talk. Bursting pain in back on coughing. Catarrh of larynx. Loss of voice. Hacking cough. Thorax feels too narrow. Cough often ends in a sneeze. Rattling in chest. Chest oppressed on ascending. Bronchial catarrh, with sore chest walls; much mucus; sensation of oppression and weight of chest. Chronic and acute bronchitis. Difficult raising of tough, profuse mucus, in the aged. Asthenic bronchitis of old people with chronic interstitial nephritis or chronic emphysema. Old asthmatics with congestive attacks. Exudations in Pleura. Hydrothorax. Pressure on chest as though lungs were forced back to spine. Voice unsteadies, vocal cords partially paralyzed.
Throat: Catarrhal inflammation of throat and faucets, with scraping hoarseness. Burning and rawness. Sensation as if membrane had been abraded.
Mercurius Sulphuricus
Throat. Heat and sensation of constriction in throat. Dryness of tongue and throat. Burning in mouth and throat. Respiratory Organs. Roughness in throat and hoarseness. Sensation of heat in larynx. Increased expectoration of mucus from larynx” and trachea. Dyspnea; in children; hydrothorax. Chronic and acute bronchitis.
Cina
Gagging cough in the morning. Whooping-cough. Violent recurring paroxysms, as of down in throat. Cough ends in a spasm. Cough so violent as to bring tears and sternal pains; feels as if something had been torn off. Periodic; returning spring and fall. Swallows after coughing. Chronic and acute bronchitis. Gurgling from throat to stomach after coughing. Child is afraid to speak or move for fear of bringing on paroxysm of coughing. After coughing, moaning, anxious, gasps for air and turns pale.
Coccus Cacti
Constant hawking from enlarged uvula; coryza, with inflamed faucets; accumulation of thick viscid mucus, which is expectorated with great difficulty. Tickling in larynx. Sensation of a crumb behind larynx, must swallow continually; brushing teeth causes cough. Faucets very sensitive. Suffocative cough; worse, first waking, with tough, white mucus, which strangles. Spasmodic morning cough. Whooping cough attacks end with vomiting of this tough mucus. Chronic and acute bronchitis complicated with gravel; large quantities of aluminous, tenacious mucus, are expectorated. Walking against wind takes breath away.
Nux Vomica
Catarrhal hoarseness, with scraping in throat. Spasmodic constriction. Asthma, with fullness in stomach, morning or after eating. Cough, with sensation as if something were torn loose in chest. Shallow respiration. Oppressed breathing. Tight, dry hacking cough; at times with bloody expectoration. Cough brings on bursting headache and bruised pain in epigastric region.
Throat: Rough, scraped feeling. Tickling after waking in morning. Sensation of roughness, tightness, and tension. Pharynx constricted. Uvula swollen. Stitches into ear.
10 home remedies for chronic cough in children and adults
- Stay hydrated. Fluids can help thin secretions.
- Gargle with warm saltwater to help cleanse the throat and rid it of mucus.
- Elevate your head with extra pillows at night to ease a chronic dry cough.
- Inhale steam in a shower or use a cool-mist humidifier to relieve dry cough.
- Cough drops may soothe an irritated throat.
- Do not smoke or use tobacco products.
- Avoid inhaled irritants such as smoke, dust, or other pollutants.
- Honey often can be an effective treatment for a persistent cough. Add honey to hot tea, or even grape juice.
- Ginger, prepared as tea, is often used to help reduce symptoms of chronic cough and clear the nasal passages.
- Other herbs such as eucalyptus or mint are often used to relieve cough symptoms.
Complications of Chronic and Acute Bronchitis
The major complications of chronic bronchitis are:
- difficulty breathing, sometimes severe,
- respiratory failure,
- pneumonia,
- Enlargement and weakness of right heart ventricle of the heart caused by lung disease,
- pneumothorax (collection of air or gas in lung causing lung collapse),
- polycythemia (abnormally high concentration of red blood cells needed to carry oxygen),
- chronic obstructive pulmonary disease
- emphysema,
- chronic advancement of the disease, and
- high mortality (death) rate.
P. S: This article is only for doctors having good knowledge about Homeopathy and allopathy, for learning purpose(s).
For proper consultation and treatment, please visit our clinic.
None of above-mentioned medicine(s) is/are the full/complete treatment but just hints for treatment; every patient has his/her own constitutional medicine.
 Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Senior research officer at Dnepropetrovsk state medical academy Ukraine.
Location: Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03059820900), K.P.K, Pakistan.
Find more about Dr Sayed Qaisar Ahmed at:
https://www.youtube.com/Dr Qaisar Ahmed
I would like to voice my passion for your kind-heartedness for all those that must have assistance with that matter. Your personal dedication to passing the solution along had become quite practical and has frequently made individuals much like me to arrive at their pursuits. Your new important guide means much a person like me and much more to my fellow workers. Warm regards; from everyone of us.