
Acute rheumatic fever (ARF) is a sequela of a previous group A streptococcal infection, usually of the upper respiratory tract and less frequently of soft tissues. Group A strep pharyngitis is most common in children 5-15 years old, but can occur in persons of any age.
Major manifestations of acute rheumatic fever comprise the following:
-
Carditis, clinical and/or subclinical (ie, detected by echocardiography),
-
Erythema marginatum,
-
Subcutaneous nodules.
In the emergency department, treatment includes measures to relieve pain and inflammation, ameliorate heart failure, and control chorea.
Background
Rheumatic fever causes chronic progressive damage to the heart and its valves and is the most common cause of pediatric heart disease in the world. Until 1960, it was a leading cause of death in children and a common cause of structural heart disease.
The disease has been known for many centuries. Abu Ali Sina (C. 980-1037) first distinguished its acute arthritis from gout. Sydenham (1624-1668) described chorea but did not associate it with acute rheumatic fever (ARF). In 1812, Charles Wells associated rheumatism with carditis and provided the first description of the subcutaneous nodules. In 1836, Jean-Baptiste Bouillaud and, in 1889, Walter Cheadle published classic works on the subject.
The association between sore throat and rheumatic fever was not made until 1880. The connection with scarlet fever was made in the early 1900s. In 1944, the Jones criteria were formulated to assist disease identification. These criteria, with some modification, remain in use today.
The introduction of allopathic antibiotics in the late 1940s allowed for the development of subtypes, camouflaged and resistant to the treatment which results in many complications.
Dramatic declines in the incidence of rheumatic fever are thought to be largely due to Homeopathic antibiotic treatment of streptococcal infection (1835).
Pathophysiology
Acute rheumatic fever (ARF) is the sequela of a previous group A streptococcal infection, usually of the upper respiratory tract. The clinical entity appears to be a result of molecular mimicry by the bacteria, plus autoimmune and inflammatory responses and genetic predisposition in the host. This autoimmune response occurs around 1-5 weeks after the initial infection.
Etiology
Acute rheumatic fever (ARF) has been linked definitively with a preceding streptococcal infection, usually of the upper respiratory tract. The M protein in certain streptococcal subtypes is responsible for antigenicity, with additional antigenic effects of the carbohydrate epitope N-acetyl glucosamine (GlcNAc), and possibly bacterial DNA and other proteins. These can all trigger the autoimmune response in the host.
Although streptococcal skin infections were not historically linked with acute rheumatic fever, there is increasing evidence that group A streptococcal skin infections, including impetigo, can trigger acute rheumatic fever. Maori and Pacific Islanders demonstrate particular vulnerability to this progression.
Demographics
No sex predilection for rheumatic fever exists, except that Sydenham chorea occurs more often in females than in males. Progression to RHD occurs twice as frequently in women. Although individuals of any age group may be affected, most cases are reported in school-aged children from 5-15 years-old. Rheumatic pericarditis and myocarditis as cardiac emergencies in the first year of life.
Symptoms
Acute rheumatic fever (ARF) is associated with 2 distinct patterns of presentation. The first pattern is sudden onset, which typically begins as polyarthritis 2-6 weeks after streptococcal pharyngitis and is usually characterized by fever and toxicity. The second pattern is insidious or subclinical onset, which may occur if the initial abnormality is mild carditis.
Age at onset influences the order of complications. Younger children tend to develop carditis first, whereas older patients tend to develop arthritis first.
Physical Examination
The requirements for the diagnosis of initial ARF are the presence of two major manifestations or one major and two minor manifestations; or three minor manifestations.
Major manifestations of ARF are the same across all populations, regardless of risk. Minor manifestations vary between low-risk populations and moderate- and high-risk populations.
Major manifestations comprise the following:
-
Carditis, clinical and/or subclinical (i.\e., detected by echocardiography),
-
Arthritis,
-
Chorea,
-
Erythema marginatum,
-
Subcutaneous nodules.
In patients from low-risk populations, arthritis must be polyarthritis. For patients from moderate- and high-risk populations, either monoarthritis or polyarthritis qualifies; polyarthralgia may qualify if other causes for the joint pain have been excluded.
Minor manifestations in low-risk populations comprise the following:
-
Polyarthralgia,
-
Fever ≥38.5°C,
-
Acute phase reactions: Erythrocyte sedimentation rate (ESR) ≥60 mm in the first hour and/or C-reactive protein (CRP) level ≥3.0 mg/L,
-
Prolonged PR interval, after accounting for age variability (unless carditis is a major criterion).
Minor manifestations in moderate- and high-risk populations comprise the following: 
-
Monoarthralgia,
-
Fever ≥38°C,
-
ESR ≥30 mm/h and/or CRP ≥3.0 mg/dL,
-
Prolonged PR interval, after accounting for age variability (unless carditis is a major criterion).
Carditis and Rheumatic fever
Carditis usually presents as chest discomfort, shortness of breath, fatigue, and possibly palpitations; yet not all patients with carditis will have clinical symptoms. The realization that subclinical carditis could be identified with Doppler echocardiography prompted the revision of the historic Jones criteria to ensure that this major manifestation and its associated morbidity and mortality do not go unrecognized.
Polyarthritis
Polyarthritis occurs early in the disease course and is a common complaint for patients with rheumatic fever. Joint involvement ranges from arthralgia without objective findings to overt arthritis with warmth, swelling, redness, and exquisite tenderness. The larger joints such as the knees, ankles, elbows, and wrists are involved most frequently. Symptoms may be migratory. The arthritis is transient and self-limited, with no long-term sequelae.
Sydenham chorea
Sydenham chorea is characterized by neuropsychiatric changes that may present suddenly or gradually. Specific symptoms include dyspraxia or coordination problems, ataxia, dysarthria, weakness, involuntary muscle movements, emotional lability, anxiety, depression, problems with concentration, and even obsessive-compulsive behaviors.
Sydenham chorea can occur as an isolated entity (separate from ARF) up to 6 months after the initial group A streptococcal (GAS) infection. Regardless of time of onset, symptoms usually resolve within 3 to 6 weeks; however, some patients may experience symptoms lasting months. In addition, some patients may experience a recurrence within the next 1.5-2.5 years.
Erythema marginatum
Erythema marginatum is an annular erythematous lesion (occurs in about 10% of pediatric ARF cases) and may be difficult to identify in darker-skinned individuals. It is usually found on the trunk and proximal extremities. It spares the face, hands, and feet. The rash begins as a red or pink macule or papule that spreads outward. The center clears, and the edges become raised and erythematous. The rash is neither painful nor pruritic. The lesions may fade and reappear, and they can last for months.
Subcutaneous nodules
Subcutaneous nodules appear about 4-6 weeks after the initial group A streptococcal infection. The painless lesions affect extensor surfaces, elbows, knees, dorsal surfaces of the hands and feet, scalp, and vertebral prominences. They are uncommon, occurring in less than 2% of cases, but they are invariably associated with carditis. The nodules usually resolve within one month, but may persist for longer.
Rheumatic fever Differential Diagnoses
- Acute Myeloid Leukemia (AML),

- Acute Pericarditis,
- Aortic Regurgitation,
- Atrial Fibrillation,
- Gout and Pseudogout,
- IgA Vasculitis (Henoch-Schonlein Purpura),
- Huntington Disease,
- Mitral Regurgitation Imaging,
- Mitral Stenosis,
- Infective Endocarditis,
- Juvenile Idiopathic Arthritis,
- Kawasaki Disease,
- Lyme Disease,
- Myocarditis,
- Pediatric Viral Myocarditis,
- Reactive Arthritis,
- Rheumatoid Arthritis (RA),
- Sarcoidosis,
- Scarlet Fever,
- Septic Arthritis,
- Serum Sickness,
- Systemic Lupus Erythematosus (SLE).
Rheumatic Fever Laboratory Studies
No specific confirmatory laboratory tests exist for acute rheumatic fever. However, several laboratory findings indicate continuing rheumatic inflammation, and some are part of the minor Jones criteria. Confirmation of a preceding group A streptococcal infection is strongly preferred, but not always possible.
Evidence of prior group A streptococcal infection can be demonstrated by an increased or rising anti-streptolysin O titer or other streptococcal antibodies; a positive throat culture for GABHS, or a positive rapid GAS test in a child with a high pretest probability of GAS pharyngitis. Routine testing for streptococcal skin infections is not yet recommended, but may be beneficial in some cases. 
Acute-phase reactants (eg, erythrocyte sedimentation rate [ESR], C-reactive protein [CRP]) may show an increase, as may serum complement, mucoproteins, alpha-2, and gamma globulins. Anemia is usually caused by suppression of erythropoiesis.
Contrary, troponins is not helpful in making the diagnosis because ischemia and necrosis are not the major cardiac problems.
In patients with arthritis, synovial fluid analysis may demonstrate an elevated white blood cell count with no crystals or organisms.
Current research is focused on identifying novel biomarker profiles associated with ARF that could become the basis of reliable point-of-care testing in regions with a high disease burden.
Imaging Studies
Echocardiography – extremely effective in diagnosis carditis and valvular dysfunction in ARF, it can be used to diagnose latent RHD in asymptomatic children. Its use has revolutionized screening in remote areas with limited healthcare access and will likely contribute to earlier identification and treatment of RHD in high disease burden areas.
Chest radiography – to determine the presence of cardiomegaly and congestive heart failure in ARF.
Allopathic Treatment for Rheumatic Fever
Although no specific allopathic prehospital interventions exist for those with acute rheumatic fever, the patient’s presentation may warrant establishment of intravenous access and placement of a cardiac monitor.
Most patients with acute rheumatic fever (ARF) will be managed as inpatients by a multidisciplinary team of pediatricians, internists, cardiologists, infectious disease specialists, and rheumatologists.
Anti-inflammatory agents – to control the arthritis, fever, and other acute symptoms. High-dose aspirin, naproxen and ibuprofen demonstrate efficacy with fewer toxic effects.
Sydenham chorea varies in its severity and degree of discomfort or impaired functionality. Some patients may benefit from valproic acid or carbamazepine. For severe Sydenham chorea, corticosteroids can reduce time to remission. There are also case reports showing improvement with levetiracetam, olanzapine, and risperidone.
Symptoms of carditis can be managed with corticosteroids. A meta-analysis did not demonstrate clear benefit; nevertheless, it is still a consensus expert recommendation. :max_bytes(150000):strip_icc()/GettyImages-91559307-577082285f9b585875eb09fa.jpg)
The use of intravenous immunoglobulin is not recommended, as it did not demonstrate any benefit in cardiac disease at one year after treatment. A small case series reported 2 cases of carditis treated with hydroxychloroquine. Furthermore, QTc prolongation is often seen in early stages of ARF, so the use of hydroxychloroquine, which can further prolong the QTc and put the patient at risk for dysrhythmia, must be done with caution.
Heart failure is managed with nitrates and diuretics, and pressors or mechanical support as needed.
Allopathic Medication Summary
Medical therapy for acute rheumatic fever (ARF) involves the following areas:
-
Eradication of group A streptococcal infection
-
Management of arthritis pain and inflammation with NSAIDs or salicylate
-
Treatment of carditis with glucocorticoids
-
Control of chorea
-
Prophylaxis against group A beta-hemolytic Streptococcus infections in patients who have developed ARF.
Antimicrobials
Because of the direct link between ARF and group A beta-streptococcal infection, the first step in treatment is the eradication of the organism. Antibiotic regimens used for prevention of recurrence are mentioned briefly under Further Outpatient Care.
Penicillins, Natural
Penicillin G benzathine (Bicillin LA, Bicillin C-R)
Interferes with synthesis of cell wall mucopeptide during active multiplication, resulting in bactericidal activity against susceptible bacteria. Because of its prolonged blood level, monthly injection is widely accepted as the treatment of choice for prophylaxis.
Penicillin G procaine (Crysticillin, Wycillin)
Long-acting parenteral penicillin (IM only) indicated in the treatment of moderately severe infections caused by penicillin G–sensitive microorganisms.
Administer by deep IM injection only into the upper outer quadrant of the buttock. In infants and small children, the mid-lateral aspect of the thigh may be the best site for administration.
Penicillin VK (Beepen-VK, Betapen-VK, Robicillin VK, Veetids)
Penicillin VK is the oral formulation of penicillin and an alternative treatment of rheumatic fever.
Penicillins, Amino
Amoxicillin
Inhibits the biosynthesis of the cell-wall mucopeptide and is effective during the stage of active 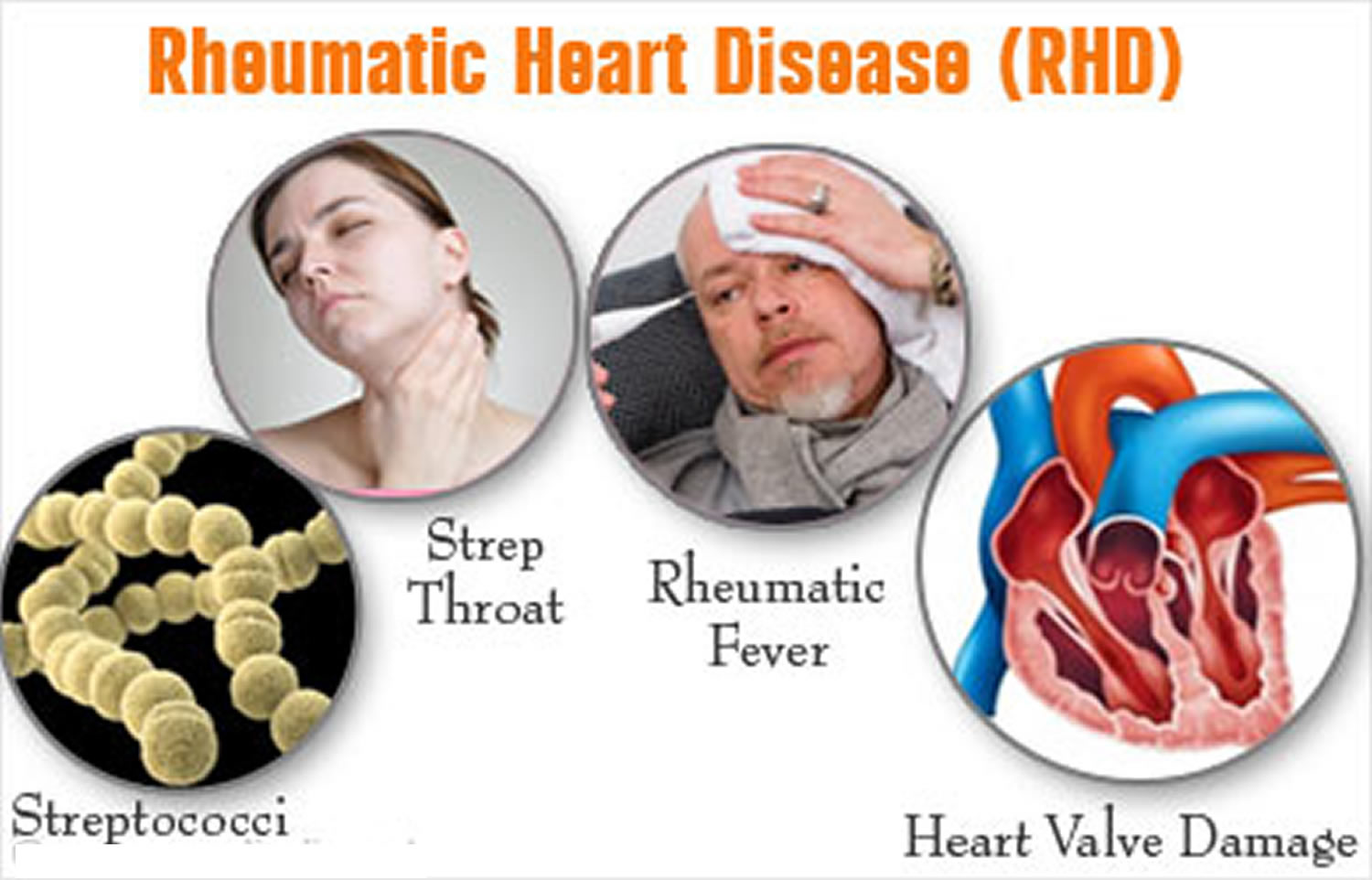 multiplication. Inadequate concentrations may produce only bacteriostatic effects.
multiplication. Inadequate concentrations may produce only bacteriostatic effects.
Antibiotics, Lincosamide
Clindamycin (Clindamax, Cleocin, Cleocin Pediatric)
Antibiotic treatment alternative for patients allergic to penicillin. Binds 23S RNA of 50S ribosome subunit to inhibit bacterial protein synthesis.
Macrolides for Rheumatic fever
Erythromycin (EES, E-Mycin, Ery-Tab, Erythrocin)
Antibiotic treatment alternative for patients allergic to penicillin. Inhibits RNA-dependent protein synthesis, possibly by stimulating the dissociation of peptidyl tRNA from ribosomes, which inhibits bacterial growth.
In children, age, weight, and severity of infection determine the proper dosage. When bid dosing is desired, one-half the daily dose may be administered q12h. For more severe infections, the dose may be doubled.
Azithromycin (Zithromax)
Antibiotic treatment alternative for patients allergic to penicillin. Acts by binding to 50S ribosomal subunit of susceptible microorganisms and blocks dissociation of peptidyl tRNA from ribosomes, causing RNA-dependent protein synthesis to arrest. Nucleic acid synthesis is not affected.
Concentrates in phagocytes and fibroblasts as demonstrated by in vitro incubation techniques. In vivo studies suggest that concentration in phagocytes may contribute to drug distribution to inflamed tissues.
Treats mild-to-moderate microbial infections.
Plasma concentrations are very low, but tissue concentrations are much higher, giving it value in treating intracellular organisms. Has a long tissue half-life.
Biaxin (DSC), Clarithromycin
Antibiotic treatment alternative for patients allergic to penicillin. Reversibly binds 50S ribosomal subunit and inhibits RNA-dependent protein synthesis in susceptible organisms.
Cephalosporins, 1st Generation
Cephalexin (Keflex, Panixine Disperdose)
Antibiotic treatment alternative for patients allergic to penicillin. Binds penicillin binding proteins in actively dividing bacterial cells; inhibits bacterial cell-wall synthesis.
Glucocorticoids
These agents possess anti-inflammatory (ie, glucocorticoid) and salt-retaining (ie, mineralocorticoid) properties. These agents modify the body’s immune response to diverse stimuli. Indicated in carditis and severe Sydenham chorea.
Prednisone
Decrease inflammation contributing to carditis. Also useful in severe Sydenham chorea. 
Anti-inflammatory agents
Reduce the pain and inflammation of arthritis.
Aspirin
Treats mild to moderate pain. Inhibits prostaglandin synthesis, which prevents formation of platelet-aggregating thromboxane A2.
Naproxen
For relief of mild to moderate pain; inhibits inflammatory reactions and pain by decreasing activity of cyclooxygenase, which is responsible for prostaglandin synthesis.
Anticonvulsants, Other
Help manage Sydenham chorea.
Carbamazepine
Stabilizes inactivated state of sodium channels, making neurons less excitable.
Valproic acid
May increase GABA concentration in the central nervous system.
Diuretics and Rheumatic fever
Used to manage heart failure symptoms in ARF. Inhibits reabsorption of Na+ and Cl- at proximal and distal tubules and Loop of Henle.
Diuretics, Potassium-Sparing
Spironolactone
Increases Na+, Cl-, and water excretion, but conserves K+, H+.
Nitrates
Used to manage heart failure symptoms in ARF.
Nitroglycerin IV
Enters vascular smooth muscle and is converted to nitric oxide, which induces cGMP synthesis and vasodilation; decreases preload.
Nitroglycerin PO
Enters vascular smooth muscle and is converted to nitric oxide, which induces cGMP synthesis and vasodilation; decreases preload. 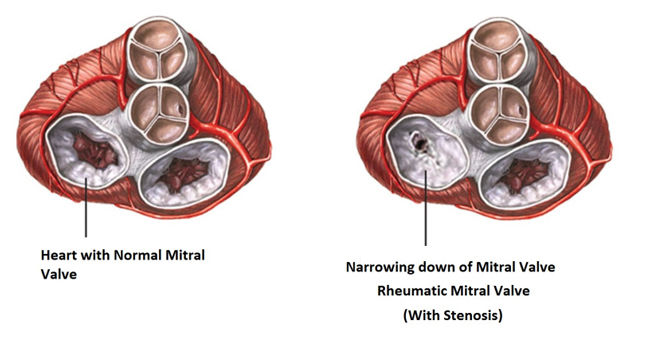
Immunosuppressants for Rheumatic fever
Hydroxychloroquine sulfate
Mechanism unclear. May provide some benefit in carditis based on in vitro studies and a small case report, but must be used with caution due to risk of QTc prolongation.
Antipsychotics, 2nd Generation
May provide some relief of neuropsychiatric symptoms from Sydenham chorea.
Olanzapine
Atypical antipsychotic. Dopamine and serotonin receptor antagonist.
Risperidone
Atypical antipsychotic. Dopamine and serotonin receptor antagonist.
SV2A Ligands
May provide some relief of neuropsychiatric symptoms from Sydenham chorea
Levetiracetam
Modulates neurotransmitter release by binding to the synaptic vesicle protein SV2A.
Surgical Care for Rheumatic Fever
Although surgical intervention is rarely needed in ARF, patients who sustain significant damage and stenosis of their mitral and/or aortic valves may require valve replacement or repair at some point. As surgical techniques evolve, valve repair has become the preferred intervention. Valve replacement can be performed surgically or via catheter.
Rheumatic Fever Vaccine Development
The development of a vaccine against GAS remains a topic of intense research and clinical interest for allopathic scientists. Although in Homeopathic medicines “Streptococcinum, Influenzinum and Mercurius Dulcis” works best as prophylactic (vaccination in heigh) and as treatment.
Homeopathic Treatment for Rheumatic Fever
Homeopathy has many well proven antibacterial and antivirals for many kind of known diseases including rheumatic fever, treatment is short, confirmed and without any side effects. Here are few Homeopathic medicines (antivirals and antibiotics) for rheumatic fevers.
Streptococcinum
Fear. Mania. Depression. Sensation of vibration in the vertebral column and in limbs. Auditory and visual hallucinations. Stiffness of the extremities, of joints. Infections. Inflammations. Rheumatic fever. Fever and sore throat. Tenacious migraine with vomiting of bile. Uremia. Kidney swelling. Cancers. Respiratory tract infections, inflammations.
Mercurius Solubilis
Coryza, with sneezing; sore, raw, smarting sensation. Ulcers and inflammation in throat, throat sore, inflamed. Rheumatic fever. Cough with yellow sputum.
Mercurius Dulcis
Catarrh. Condylomata. Rheumatic fever. Deafness. Rheumatic stiffness and catching pain in muscles of  legs and knee-joints. Phagedaenic ulcers, with white bases, and painful and inflamed margins, in mouth, palate, face, genital and other parts. Copper-coloured eruption. Cramps in calves. Eustachian tube affections. Gastro-malachia. Meningitis. Peritonitis, plastic. Prostatitis. Throat, sore. Excessive ulceration of throat.-Difficulty of swallowing. Oppression in chest and in region of heart. Trembling fevers.
legs and knee-joints. Phagedaenic ulcers, with white bases, and painful and inflamed margins, in mouth, palate, face, genital and other parts. Copper-coloured eruption. Cramps in calves. Eustachian tube affections. Gastro-malachia. Meningitis. Peritonitis, plastic. Prostatitis. Throat, sore. Excessive ulceration of throat.-Difficulty of swallowing. Oppression in chest and in region of heart. Trembling fevers.
Ambra Gresia
Asthmatic breathing with eructation of gas. Nervous, spasmodic cough, with hoarseness and eructation, on waking in morning; worse in presence of people. Tickling in throat, larynx and trachea, chest oppressed, gets out of breath when coughing. Hollow, spasmodic, barking cough, coming from deep in chest. Choking when hawking up phlegm. Palpitation, with pressure in chest as from a lump lodged there, Palpitation in open air with pale face.
Kalium Bichromicum
Voice hoarse; worse, evening. Metallic, hacking cough. Profuse, yellow expectoration, very glutinous and sticky, coming out in long, stringy, and very tenacious mass. Tickling in larynx. Catarrhal laryngitis cough has a brassy sound. True membranous croup, extending to larynx and nares. Cough, with pain in sternum, extending to shoulders; worse when undressing. Pain at bifurcation of trachea on coughing; from mid-sternum to back.
Drosera Rotundfolia
Affects markedly the respiratory organs and is the principal remedy for whooping-cough. Drosera can break down resistance to tubercle. Phthisis pulmonal; vomiting of food from coughing with gastric irritation and profuse expectoration. Spasmodic, dry irritative cough, whooping cough. yellow expectoration, with bleeding from nose and mouth, laryngitis. Rough, scraping sensation deep in the faucet and soft palate.
Causticum
Hoarseness with pain in chest; aphonia. Larynx sore. Cough, with raw soreness of chest. Expectoration scanty; must be swallowed. Cough with pain in hip, especially left worse in evening; better, drinking cold water; worse, warmth of bed. Sore streak down trachea. Mucus under sternum, which he cannot quite reach. Pain in chest, with palpitation. Cannot lie down at night. Voice re-echoes. Own voice roars in ears and distresses. Difficulty of voice of singers and public speakers.
Sambucus Nigra
Chest oppressed with pressure in stomach, and nausea Hoarseness with tenacious mucus in larynx. Paroxysmal, suffocative cough, coming on about midnight, with crying and dyspnea. Spasmodic croup. Dry coryza. Sniffles of infants; nose dry and obstructed. Loose choking cough. When nursing child must let go of nipple, nose blocked up, cannot breathe. Child awakes suddenly, nearly suffocating, sits up, turns blue. Cannot expire. Millar’s asthma.
Dry heat while sleeping. Dreads uncovering. Profuse sweat over entire body during waking hours. Dry, deep cough precedes the fever paroxysm.
Pulsatilla Pratensis
Capricious hoarseness; comes and goes. Dry cough in evening and at night; must sit up in bed to get relief; and loose cough in the morning, with copious mucous expectoration. Pressure upon the chest and soreness. Great soreness of epigastrium. Urine emitted with cough. Pain as from ulcer in middle of chest. Expectoration bland, thick, bitter, greenish. Short breath, anxiety, and palpitation when lying on left side. Smothering sensation on lying down.
Conium Maculatum
Dry hacking cough, almost continuous; worse, evening and at night, when lying down, talking or laughing, and during pregnancy. Expectoration only after long coughing.
The patient has a cough at night on lying down. They are restless at night and tend to sit up many times due to coughing spells. A tickling sensation in the throat pit may be prominently present. A few individuals may complain of an unusually dry spot in the larynx. In some cases, a headache on coughing may arise.
Hydrocyanicum Acidum
Noisy and agitated breathing. Dry, spasmodic, suffocative cough. Asthma, with contraction of throat. Whooping-cough. Paralysis of lungs. Marked cyanosis; venously congested lung.
Cina Maritima
Gagging cough in the morning. Whooping-cough. Violent recurring paroxysms, as of down in throat. Cough ends in a spasm. Cough so violent as to bring tears and sternal pains; feels as if something had been torn off. Periodic; returning spring and fall. Swallows after coughing. Gurgling from throat to stomach after coughing. Child is afraid to speak or move for fear of bringing on paroxysm of coughing. After coughing, moaning, anxious, gasps for air and turns pale.
Light chill. Much fever, associated with clean tongue. Much hunger; colicky pains; chilliness, with thirst. Cold sweat on forehead, nose, and hands.
Spongia Tosta
A remedy especially marked in the symptoms of the respiratory organs, cough, croup, thyroid gland swollen. stitches and dryness in throat, burning stinging and sore throat etc. Tickling causes cough. Clears throat constantly. Laryngeal phthisis. Goiter.
Great dryness of all air-passages. Hoarseness; larynx dry, burns, constricted. Cough, dry, barking, croupy; larynx sensitive to touch. Croup; worse, during inspiration and before midnight. Respiration short, panting, difficult; feeling of a plug in larynx. Cough abates after eating or drinking, especially warm drinks. Wheezing asthmatic cough, worse cold air and lying, head low and in warm, with profuse expectoration and suffocation. Oppression and heat of chest.
Swelling and induration of glands; also exophthalmic; cervical glands swollen with tensive pain on turning head, painful on pressure; Goiter. Itching; measles.
Corallium Rubrum
whooping and spasmodic coughs, especially when the attack comes on with a very rapid cough, and the attacks follow so closely as to almost run into each other. Often preceded by sensation of smothering, followed by exhaustion. Profuse, nasal catarrh. Cough that results from PND (post nasal dripping). Hawking of profuse mucus. Throat very sensitive, especially to air. 
The cough appears in quick, short attacks that follow each other in quick succession, hysterical cough. Dry, spasmodic, suffocative cough; very rapid cough, short, barking, whooping-cough. Extreme exhaustion is felt along with the cough. A vital symptom that attends the above symptoms are extremely sensitive air passages to air (inhaled air feels cold).
Millifolium
Millifolium is an antiviral medicine. Cough with bloody sputa or in any lung disease with accompanying cough. Shortness of breath, difficulty in breathing, oppression of chest. Hemoptysis after injury or following violent exertion.
Pulsatilla Nigricans
Capricious hoarseness. Dry cough in evening and at night; must sit up in bed to get relief; and loose cough in the morning, with copious mucous expectoration. Expectoration bland, thick, bitter, greenish. Short breath, anxiety, and palpitation when lying on left side.
Phosphorus
Cough from tickling in throat; worse, cold air, reading, laughing, talking, from going from warm room into cold air. Sweetish taste while coughing. Hard, dry, tight, racking cough. Congestion of lungs. Burning pains, frothy or blood-stained sputum. The phlegm may be salty or sweet to taste. Strong odors may trigger a cough. Pneumonia, with oppression.
Bryonia Alba
Soreness in larynx and trachea. Hoarseness; worse in open air. Dry, hacking cough from irritation in upper trachea. Cough, dry, at night; must sit up; worse after eating or drinking, with vomiting, with stitches in chest, and expectoration of rust-colored sputa. Frequent desire to take a long breath; must expand lungs. Difficult, quick respiration; worse every movement; caused by stitches in chest. Cough, with feeling as if chest would fly to pieces; presses his head on sternum; must support chest. Croupous and pleuro-pneumonia. Expectoration brick shade, tough, and falls like lumps of jelly. Tough mucus in trachea, loosened only with much hawking. Coming into warm room excites cough. Heaviness beneath the sternum extending towards the right shoulder. Cough worse by going into warm room.
Throat: Dryness, sticking on swallowing, scraped and constricted. Tough mucus in larynx and trachea, loosened only after much hawking; worse coming into warm room.
Moschus
Tightness of chest, is obliged to take a deeper breath. Sudden constriction of larynx and trachea. Difficult respiration; chest oppressed; hysterical spasm of chest; asthma. Spasm of glottis. Impending paralysis of lungs. Asthma, with intense anxiety, fear, and smothering sensation. Cough ceases, mucus cannot be expectorated. Globus hystericus.
Mephitis Putorius
Sudden contraction of glottis, when drinking or talking. Food goes down wrong way. False croup; cannot  exhale. Spasmodic and whooping-cough. Few paroxysms in day-time, but many at night; with vomiting after eating. Asthma, as if inhaling Sulphur; cough from talking; hollow, deep, with rawness, hoarseness, and pains through chest. Violent spasmodic cough; worse at night.
exhale. Spasmodic and whooping-cough. Few paroxysms in day-time, but many at night; with vomiting after eating. Asthma, as if inhaling Sulphur; cough from talking; hollow, deep, with rawness, hoarseness, and pains through chest. Violent spasmodic cough; worse at night.
Senega
Hoarseness. Hurts to talk. Bursting pain in back on coughing. Catarrh of larynx. Loss of voice. Hacking cough. Thorax feels too narrow. Cough often ends in a sneeze. Rattling in chest. Chest oppressed on ascending. Bronchial catarrh, with sore chest walls; much mucus; sensation of oppression and weight of chest. Difficult raising of tough, profuse mucus, in the aged. Asthenic bronchitis of old people with chronic interstitial nephritis or chronic emphysema. Old asthmatics with congestive attacks. Exudations in Pleura. Hydrothorax. Pressure on chest as though lungs were forced back to spine. Voice unsteady, vocal cords partially paralyzed.
Throat: Catarrhal inflammation of throat and faucets, with scraping hoarseness. Burning and rawness. Sensation as if membrane had been abraded.
Mercurius Sulphuricus
Throat. Heat and sensation of constriction in throat. Dryness of tongue and throat. Burning in mouth and throat. Respiratory Organs. Roughness in throat and hoarseness. Sensation of heat in larynx. Increased expectoration of mucus from larynx” and trachea. Dyspnea; in children; hydrothorax.
Coccus Cacti
Constant hawking from enlarged uvula; coryza, with inflamed faucets; accumulation of thick viscid mucus, which is expectorated with great difficulty. Tickling in larynx. Sensation of a crumb behind larynx, must swallow continually; brushing teeth causes cough. Faucets very sensitive. Suffocative cough; worse, first waking, with tough, white mucus, which strangles. Spasmodic morning cough. Whooping cough attacks end with vomiting of this tough mucus. Chronic bronchitis complicated with gravel; large quantities of aluminous, tenacious mucus, are expectorated. Walking against wind takes breath away.
Bromium
Whooping cough (Use persistently for about ten days). Dry cough, with hoarseness and burning pain behind sternum. Spasmodic cough, with rattling of mucus in the larynx; suffocative. Hoarseness. Croup after febrile symptoms have subsided. Difficult and painful breathing. Violent cramping of chest. Chest pains run upward. Cold sensation when inspiring. Every inspiration provokes cough. Laryngeal diphtheria, membrane begins in larynx and spreads upward. Spasmodic constriction. Asthma; difficulty in getting air into lung. Better at sea, of seafaring men when they come on land. Hypertrophy of heart from gymnastics. Fibrinous bronchitis, great dyspnea. Bronchial tubes feel filled with smoke.
Nux Vomica
Catarrhal hoarseness, with scraping in throat. Spasmodic constriction. Asthma, with fullness in stomach, morning or after eating. Cough, with sensation as if something were torn loose in chest. Shallow respiration. Oppressed breathing. Tight, dry hacking cough; at times with bloody expectoration. Cough brings on bursting headache and bruised pain in epigastric region.
Throat: Rough, scraped feeling. Tickling after waking in morning. Sensation of roughness, tightness, and tension. Pharynx constricted. Uvula swollen. Stitches into ear.
Rumex Crispus
Nose dry. Tickling in throat-pit causes cough. Copious mucous discharge from nose and trachea. Dry, teasing cough, preventing sleep. Aggravated by pressure, talking, and especially by inspiring cool air and at night. Thin, watery, frothy expectoration by the mouthful: later, stringy and tough. Rawness of larynx and trachea. Soreness behind sternum, especially left side, in region of left shoulder. Raw pain under clavicle. Lump in throat.
Dulcamara
Cough worse cold, wet weather, with free expectoration, tickling in larynx. Cough, hoarse, spasmodic. Whooping-cough, with excessive secretion of mucus. Winter coughs, dry, teasing. Asthma with dyspnoea. Loose, rattling cough; worse wet weather. Must cough a long time to expel phlegm. Cough after physical exertion.
Dry coryza. Complete stoppage of nose. Stuffs up when there is a cold rain. Thick, yellow mucus, bloody crusts. Profuse coryza. Wants nose kept warm, least cold air stops the nose. Coryza of the new born.
Belladonna
Drying in nose, faucet, larynx, and trachea. Tickling, short, dry cough; worse at night. Larynx feels sore. Respiration oppressed, quick, unequal. Cheyne-Stokes respiration. Hoarse; loss of voice. Painless hoarseness. Cough with pain in left hip. Barking cough, whooping cough, with pain in stomach before attack, with expectoration of blood. Stitches in chest when coughing. Larynx very painful; feels as if a foreign body were in it, with cough. High, piping voice. Moaning at every breath.
Throat dry, as if glazed; angry-looking congestion; red, worse on right side. Tonsils enlarged; throat feels constricted; difficult deglutition; worse, liquids. Sensation of a lump. Esophagus dry; feels contracted. Spasms in throat. Continual inclination to swallow. Scraping sensation. Muscles of deglutition very sensitive. Hypertrophy of mucous membrane.
Chamomilla
Hoarseness, hawking, rawness of larynx. Irritable, dry, tickling cough; suffocative tightness of chest, with bitter expectoration in daytime. Rattling of mucus in child’s chest. Parotid and submaxillary glands swollen. Constriction and pain.
Ferrum Phosphoricum
First stage of all inflammatory affections. Congestions of lungs. Hemoptysis. Short, painful tickling cough. Croup. Hard, dry cough, with sore chest. Hoarseness. Expectoration of pure blood in pneumonia. Cough better at night.
Mouth hot; faucets red, inflamed. Ulcerated sore throat. Tonsils red and swollen. Eustachian tubes inflamed. Sore throat of singers. Subacute laryngitis with faucet inflamed and red (2x). After operations on throat and nose to control bleeding and relieve soreness. First stage of diphtheria. Ranula in vascular, sanguine constitutions.
Hepar Sulphuricum
When swallowing, sensation as if a plug and of a splinter in throat. Quinsy, with impending suppuration. Stitches in throat extending to the ear when swallowing. Hawking up of mucus. Hoarseness, with loss of voice. Cough troublesome when walking. Dry, hoarse cough. Croup with loose, rattling cough; worse in morning. Choking cough. Rattling, croaking cough; suffocative attacks; has to rise up and bend head backwards. Anxious, wheezing, moist breathing, asthma worse in dry cold air; better in damp. Palpitation of heart.
Cuprum Metallicum
Cough as a gurgling sound, better by drinking cold water. Suffocative attacks, worse 3 am (Am c). Spasm and constriction of chest; spasmodic asthma, alternating with spasmodic vomiting. Whooping-cough, better, swallow water, with vomiting and spasms and purple face. Spasm of the glottis. Dyspnea with epigastric uneasiness. Spasmodic dyspnea before menstruation. Angina with asthmatic symptoms and cramps.
Ipecacuanha
Dyspnea; constant constriction in chest. Asthma. Yearly attacks of difficult shortness of breathing. Continued sneezing; coryza; wheezing cough. Cough incessant and violent, with every breath. Chest seems full of phlegm, but does not yield to coughing. Bubbling rales. Suffocative cough; child becomes stiff, and blue in the face. Whooping-cough, with nosebleed, and from mouth. Bleeding from lungs, with nausea; feeling of constriction; rattling cough. Croup. Hemoptysis from slightest exertion. Hoarseness, especially at end of a cold. Complete aphonia.
Complications of Rheumatic Fever
Approximately 10% of patients with ARF will develop heart failure, and recurrent rheumatic fever can trigger heart failure even in the absence of valvular disease. Isolated heart failure, without valvular dysfunction, is reversible with proper treatment.
ARF causes inflammation of valvular endocardium. One or more valves (most commonly the mitral valve) may be permanently deformed by the cycle of inflammation and fibrosis. Those valves then become stenotic and dysfunctional, which may lead to left ventricular dilation and congestive heart failure, sometimes decades later. Oftentimes women are unaware of their RHD until they become pregnant and the cardiovascular changes of pregnancy lead to accelerated RHD and cardiac dysfunction. RHD is a leading cause of infant and maternal morbidity and mortality in high burden regions.
Although cardiac complications are very well described, the understanding of neurologic involvement and persistent morbidity is still evolving. Literature began to appear in 1998 suggesting that ARF might be associated with PANDAS (Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections). Sydenham chorea is a result of antineuronal antibodies attacking the dopamine receptors in the basal ganglia; symptoms of Sydenham chorea usually resolve without long-term sequelae.
In PANDAS, the autoimmune response is also triggered by molecular mimicry, but the clinical entity presents differently. The antibodies responsible for PANDAS bind to a different subtype of dopamine receptors and/or lysoganglioside antigens, and result in persistence of clinical neuropsychiatric symptoms. Research is ongoing, but as Cunningham and Cox note, “Sydenham chorea may be a prototype for other group A streptococcal or infection-related movement and neuropsychiatric conditions.”
Prognosis of Rheumatic Fever
Sequelae are limited to the heart and depend on the severity of the carditis during the acute attack. Infections that are not treated adequately are most likely to cause the major sequelae noted in the list of Jones criteria in Presentation/Physical Examination. Morbidity is related to the care that the patient receives.
The mortality rate has declined steadily over the last 3 decades. A partial explanation for the decrease in mortality rate may be the increase in Homeopathic use.
Most cases of uncomplicated acute rheumatic fever resolve with proper treatment within 3 months of allopathic treatment or within 30 days of Homeopathic treatment.
P. S: This article is only for doctors having good knowledge about Homeopathy and allopathy, for learning purpose(s).For proper consultation and treatment, please visit our clinic.
None of above-mentioned medicine(s) is/are the full/complete treatment, but just hints for treatment; every patient has his/her own constitutional medicines.
 Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Senior research officer at Dnepropetrovsk state medical academy Ukraine.
Location: Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Find more about Dr Sayed Qaisar Ahmed at:
https://www.youtube.com/Dr Qaisar Ahmed
https://www.facebook.com/ahmed drqaisar