
Parinaud’s syndrome is also known as sylvian aqueduct syndrome, dorsal midbrain syndrome, pretectal syndrome, and Koerber-Salus-Elschnig syndrome.
Parinaud’s syndrome results from midbrain trauma. The pupils are mid-dilated and fixed, convergence is not impaired, and there is paresis of upward gaze. Parinaud syndrome is classically described by the triad of impaired upward gaze, convergence retraction nystagmus, and pupillary hyporeflexia.
Parinaud’s midbrain syndrome is a form of ophthalmoplegia involving the internal neuromuscular mechanism of the eye, with hypertonicity and paresis of pupillary constriction and accommodation. It typically results from damaged premotor pathways for binocular upward gaze in the dorsal mesencephalon.
The most common causes of Parinaud’s syndrome are pineal gland tumors and midbrain infarction. Neoplasms, vascular occlusions, trauma, extra-axial and intra-axial arteriovenous malformations, demyelination, giant aneurysms of the posterior fossa, infections, trauma, stereotactic surgery for pain, and hydrocephalus from various causes have also been associated with Parinaud’s syndrome.
Clinical presentation
Parinaud’s syndrome is characterized by a classic triad of findings:
- Upward gaze palsy, often manifesting as diplopia.
- Pupillary light-near dissociation (pupils respond to near stimuli, but not light).
- Convergence-retraction nystagmus.
Other clinical features which may be present:
- Bilateral upper eyelid retraction (Collier sign).
- Downbeat nystagmus.
Ocular Symptoms and Signs 
Ocular signs of Parinaud’s syndrome include bilateral eyelid retraction without lagophthalmos and limitation of upgaze (supraduction). Skew deviation, head tilt, and deviation of the subjective visual vertical have been reported. Light-near dissociation is typical (i.e., the pupils constrict more when the eyes converge than in response to a light stimulus). Vertical voluntary saccades are also affected, and vertical smooth pursuit and vestibular eye movements are sometimes affected, depending on the involvement of the interstitial nucleus of Cajal. Other associated ocular signs include pseudo abducens palsy, convergence-retraction nystagmus, spasm or paresis of convergence, and spasm or paresis of accommodation. With obstruction of the aqueduct, internal hydrocephalus develops, and papilledema may be found.
Diagnosis
Neuroimaging (MRI with gadolinium) is essential to look for hydrocephalus, stroke, tumor, infection, and other structural lesions.
Allopathic Treatment and Management for Parinaud’s syndrome
Allopathic treatment for Parinaud’s syndrome is primarily directed towards etiology of the dorsal midbrain syndrome. After thorough workup, including neuroimaging it is essential to rule out anatomic lesions or other causes of this syndrome. Allopathically visually significant upgazed palsy can be relieved only with bilateral inferior rectus recessions. Retraction nystagmus and convergence movements are sometimes improved with this procedure as well.
Those patients who do not show improvement within this time are assumed not to have potential for subsequent progress. A patient’s improvement depends on the nature and extent of the damage in addition to the duration between onset of the condition and treatment. If dysmotility persists after treatment/sugary of the underlying cause, surgery on the eye muscles can be performed to achieve single vision.
Scientists are still working on proper and effective treatment for Parinaud’s syndrome.
Homeopathic treatment for Parinaud’s syndrome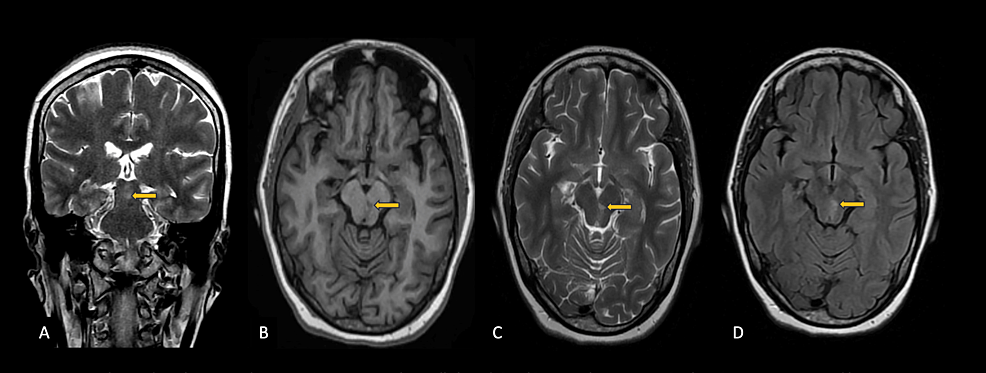
Homeopathic treatments are not to focus on only symptom but to treat the root cause along with the symptoms. Treatment of Parinaud’s syndrome is directed at treatment of the underlying disease and ophthalmic complaints. For example, vascular etiologies such as stroke could be treated with Homeopathic medicines. Niemann-Pick Disease Type C could be treated with Homeopathy. Homeopathic treatment for Parkinson’s Disease may cure ophthalmic manifestations such as saccadic accuracy and smooth pursuit.
Note: To shorten the article for your convenience, for each disease Homeopathic treatment please click the specific link given above.
Prognosis
The prognosis for Parinaud’s syndrome depends on the underlying etiology and treatment type; in allopathy there is no cure for Parinaud’s syndrome, on the other hand Homeopathy can easily handle and cure Parinaud’s syndrome and its root causes (central nervous system {Stroke, Parkinson’s disease etc.}, Neiman Pick disease etc.) in 30-90 days.
If allopathic medication is provoking the symptoms, improvement may be seen after medication discontinuation (not sure). Similarly, allopathic treatment of a compressive lesion or lowering of elevated intracranial pressure may result in improvement. The condition can be permanent due to the irreversible nature of the lesion in many cases. Allopath thinks that neurodegenerative disease (e.g., PSP) typically exhibits slow progression, Homeopathy proves it wrong.
P. S: This article is only for doctors having good knowledge about Homeopathy and allopathy, for learning purpose(s).
For proper consultation and treatment, please visit our clinic.
None of above-mentioned medicine(s) is/are the full/complete treatment, but just hints for treatment; every patient has his/her own constitutional medicine.
To order medicine by courier, please send your details at WhatsApp– +923119884588
 Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Senior research officer at Dnepropetrovsk state medical academy Ukraine.
Location: Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Find more about Dr Sayed Qaisar Ahmed at:
https://www.youtube.com/Dr Qaisar Ahmed
Do you mind if I quote a couple of your posts as long as I provide credit and sources back to your site? My blog site is in the exact same niche as yours and my visitors would definitely benefit from a lot of the information you present here. Please let me know if this alright with you. Cheers!
hi!,I like your writing very much! percentage we communicate more about your post on AOL? I require an expert in this area to solve my problem. May be that’s you! Taking a look forward to peer you.
you’re really a good webmaster. The web site loading speed is incredible. It seems that you are doing any unique trick. Also, The contents are masterpiece. you’ve done a magnificent job on this topic!
Hi there, just became aware of your blog through Google, and found that it is truly informative. I抦 gonna watch out for brussels. I抣l appreciate if you continue this in future. Many people will be benefited from your writing. Cheers!
I think this is among the most important info for me. And i’m glad reading your article. But should remark on few general things, The web site style is ideal, the articles is really nice : D. Good job, cheers
I’ve been absent for a while, but now I remember why I used to love this site. Thank you, I will try and check back more often. How frequently you update your site?
Hello. excellent job. I did not anticipate this. This is a remarkable story. Thanks!