
Ovarian cysts are closed, sac-like structures within an ovary that contain a liquid, or semi solid substance. “Cyst” is merely a general term for a fluid-filled structure, which may or may not represent a tumor or neoplasm (new growth). If it is a tumor, it may be benign or malignant. The ovary is also referred to as the female gonad. There are many causes of ovarian cysts, and most ovarian cysts are not cancerous.
Ovarian cysts may not cause signs or symptoms, but larger cysts are more likely to cause signs and symptoms such as:
Most ovarian cysts are never noticed and resolved without women ever realizing that they are there. When a cyst causes symptoms, pain in the abdomen or pelvis is the most common one. The pain can be caused from:
- rupture of the cyst,
- rapid growth and stretching,
- bleeding into the cyst, or
- twisting of the cyst around its blood supply (known as torsion).
If the cyst has reached a large size, other symptoms may arise as a result of pressure or distortion of adjacent anatomical structures. These other symptoms can include:
- abdominal fullness, expansion of the abdomen, or bloating,
- low back pain,
- indigestion,
- feeling full after eating only a small amount (early satiety),
- urinary urgency,
- difficulty with emptying the bladder,
- feeling an urge to defecate
- having difficult bowel movements, or
- pain with sexual intercourse.
What are the symptoms of a ruptured ovarian cyst?
A ruptured (burst) ovarian cyst will not always cause symptoms, particularly if the cyst is small. However, sometimes a ruptured ovarian cyst can lead to severe pain and internal bleeding. The pain with a ruptured ovarian cyst typically comes on suddenly and occurs on one side only. The pain may begin during physical activity such as vigorous exercise or may begin during sexual intercourse. A ruptured ovarian cyst usually does not cause fever or gastrointestinal symptoms.
Types of ovarian cysts
- Follicular cysts: The most common type is a follicular cyst, which results from the growth of a
 follicle. A follicle is the normal fluid-filled sac that contains an egg. Follicular cysts form when the follicle grows larger than normal during the menstrual cycle and does not open to release the egg. Usually, follicular cysts resolve on their own for days to months. Follicular cysts can contain blood (hemorrhagic cysts) from leakage of blood into the egg sac.
follicle. A follicle is the normal fluid-filled sac that contains an egg. Follicular cysts form when the follicle grows larger than normal during the menstrual cycle and does not open to release the egg. Usually, follicular cysts resolve on their own for days to months. Follicular cysts can contain blood (hemorrhagic cysts) from leakage of blood into the egg sac. - Corpus luteum cysts: A Corpus luteum cyst is related to the menstrual cycle. The corpus luteum
is an area of tissue within the ovary that occurs after an egg has been released from a follicle. If a pregnancy doesn’t occur, the corpus luteum usually breaks down and disappears. It may, however, fill with fluid or blood and persist as a cyst on the ovary. Usually, this cyst is found on only one side, produces no symptoms, and resolves spontaneously.
- “Chocolate cysts:” Endometriosis is a condition in which cells that normally grow inside as a lining of the uterus (womb), instead grow outside of the uterus in other locations. The ovary is a common site for endometriosis. When endometriosis involves the ovary, the area of endometrial tissue may grow and bleed over time, forming a blood-filled cyst with red- or brown-colored contents called an endometrioma, sometimes referred to as a “chocolate cyst.”
- Polycystic ovarian syndrome: The condition known as a polycystic ovarian syndrome (PCOS)
 is characterized by the presence of multiple small cysts within both ovaries. PCOS is associated with several hormonal problems and is the most common cause of infertility in women.
is characterized by the presence of multiple small cysts within both ovaries. PCOS is associated with several hormonal problems and is the most common cause of infertility in women. - Dermoid cysts (benign cystic teratomas): Both benign and malignant tumors of the ovary may also be cystic. Occasionally, the tissues of the ovary develop abnormally to form other body tissues such as hair or teeth. Cysts with these abnormal tissues are tumors called benign cystic teratomas or dermoid cysts.
- Tubo-ovarian abscesses: Infections of the pelvic organs can involve the ovaries and Fallopian tubes. In severe cases, pus-filled cystic spaces may be present on, in, or around the ovary or tubes. These are known as tube-ovarian abscesses.
Can some types of ovarian cysts cause cancer?
Most ovarian cysts are not due to cancer, and having an ovarian cyst does not cause ovarian cancer. However, some ovarian cancers develop cystic areas inside the tumor. Ovarian cancer is much less common than benign ovarian cysts.
Ovarian cysts during pregnancy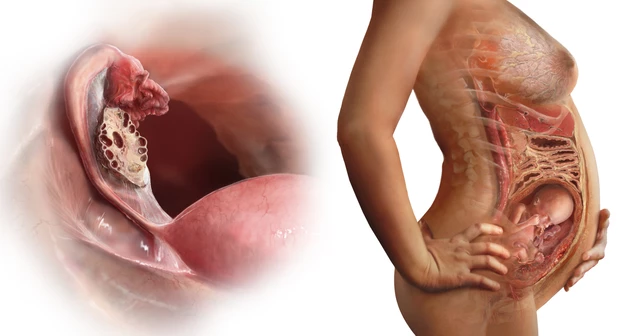
Ovarian cysts are sometimes discovered during pregnancy. In most cases, they are an incidental finding at the time of routine prenatal ultrasound screening. The majority of ovarian cysts found during pregnancy are benign conditions that do not require surgical intervention. However, surgery may be indicated if there is a suspicion of malignancy, if an acute complication such as rupture or torsion (twisting of the cyst, disrupting the blood supply) develops, or if the size of the cyst is likely to present problems with the pregnancy.
Ovarian cysts during menopause or postmenopause
Ovarian cysts may develop during pregnancy or at any point in a woman’s life. Some kinds of ovarian cysts are related to the menstrual cycle and occur before a woman has reached menopause (the time point at which a woman has not had a menstrual period for 12 consecutive months). However, postmenopausal women may still develop other types of ovarian cysts.
Diagnosis
Sometimes ovarian cysts may be noticed by a doctor during a bimanual examination of the pelvis. If a cyst is suspected based upon symptoms or physical examination, imaging techniques are used. Most cysts are diagnosed by ultrasound, which is the best imaging technique for detecting them. Ultrasound uses sound waves to produce an image of structures within the body. Ultrasound imaging is painless and harmless. Transvaginal ultrasound is a diagnostic tool to better visualize the ovaries using a thin ultrasound probe inside the vagina.
Cysts can also be detected with other imaging methods, such as a CT scan or MRI scan (magnetic resonance imaging).
Functional ovarian cysts
If a woman is in her 40’s, or younger, and has regular menstrual periods, most ovarian masses are “functional ovarian cysts,” which are not abnormal. Examples include follicular cysts and corpus luteum cysts. These are related to the process of ovulation that happens with the menstrual cycle. They usually disappear on their own during a future menstrual cycle. Therefore, especially in women in their 20s and ’30s, these cysts are watched for a few menstrual cycles to verify that they disappear.
Because oral contraceptives work by preventing ovulation, physicians will not generally expect women who are taking oral contraceptives to have common “functional ovarian cysts.” These women do not have functional ovarian cysts. They may receive a further evaluation with pelvic ultrasound or possibly surgical intervention. Functional ovarian cysts do not occur in women after they have reached menopause. Small cystic arrested follicles may persist in the ovary after menopause.
Other factors help evaluate ovarian cysts (besides the woman’s age, or whether she is taking oral contraceptives). A cyst that contains a simple sack of fluid on ultrasound is more likely to be a benign neoplasm than a cyst with solid tissue in it. So the ultrasound appearance also plays a role in determining the level of suspicion regarding an ovarian tumor.
Cancer risks
Ovarian cancer is rare in women younger than age 40. After age 40, an ovarian cyst has a higher chance of being cancerous than before age 40, although most ovarian cysts are still benign even after age 40. CA-125 blood testing can be used as a marker of ovarian cancer, but it does not always represent cancer, even when it is abnormal, and it may be normal in the presence of malignancy. CA-125 is a protein that is elevated in the bloodstream of many women with advanced ovarian cancer.
First, many benign conditions in women of childbearing age can cause the CA-125 level to be elevated, so CA-125 is not a specific test, especially in younger women. Pelvic infections, uterine fibroids, pregnancy, benign (hemorrhagic) ovarian cysts, endometriosis, and liver disease are some of the conditions that may elevate blood CA-125 levels in the absence of ovarian cancer.
Second, even if the woman has ovarian cancer, not all ovarian cancers will cause the CA-125 level to be elevated. Furthermore, CA-125 levels can be abnormally high in women with breast, lung, and pancreatic cancer.
Allopathic treatment for all types of ovarian cysts
Most ovarian cysts in women of childbearing age are follicular or corpus luteum cysts (functional cysts) that disappear naturally in one to three months, although they can rupture and cause pain. They are benign and have no long-term medical consequences. They may be diagnosed incidentally during a pelvic examination in women who do not have any related symptoms. All women have follicular cysts at some point that generally go unnoticed.
Ultrasound is useful to determine if the cyst is simple (just fluid with no solid tissue, suggesting a benign condition) or compound (with solid components that often require surgical resection).
In summary, the ideal treatment of ovarian cysts depends on the likely cause of the cysts and whether or not it is producing symptoms. The woman’s age, the size (and any change in size) of the cyst, and the cyst’s appearance on ultrasound help determine the treatment. Functional cysts are usually observed (watchful waiting) with frequent monitoring unless they rupture and cause significant bleeding, in which case, surgical treatment is required. Benign and malignant tumors require an operation.
Treatment can consist of simple observation, or it can involve evaluating blood tests such as a CA-125 to help determine the potential for cancer (keeping in mind the many limitations of CA-125 testing described above).
There are no natural or home remedies to treat ovarian cysts, other than taking non-steroidal anti-inflammatory drugs for pain management.
Surgery for ovarian cysts
Any type of ovarian mass, including a cyst, can be surgically removed either with laparoscopy, or if needed, an open abdominal incision (laparotomy) if it is causing severe pain, not resolving, or if it is suspicious in any way. Once the cyst is removed, the growth is sent to a pathologist who examines the tissue under a microscope to make the final diagnosis as to the type of cyst present.
Homeopathic Treatment for different types of ovarian cysts
Baryta Carbonica
Diminution of sexual desire in women. Cysts. Catamenia too feeble, and of too short duration. Leucorrhoea a little before the catamenia. Swelling and induration of the glands. Tumours. Warts.
Lachesis Muta
Lachesis Muta is best for left sided ovarian cysts. Swelling and pain in the left ovary that gets better during menses, short and scanty menses, and menstrual bleeding that is blackish in color. Climacteric troubles, palpitation, flashes of heat, hemorrhages, vertex headache, fainting spells; worse, pressure of clothes. Menses too short, too feeble; pains all relieved by the flow. Left ovary very painful and swollen, indurated. Mammae inflamed, bluish. Coccyx and sacrum pain (ovarian cysts), especially on rising from sitting posture. Acts especially well at beginning and close of menstruation.
Eupionum
Amenorrhea. Cramps. Glandular swellings. Groins, pain in. Hemorrhages. Headache. Leucorrhea. Menorrhagia. Neuralgia. Night-sweats. Phthisis. Pruritus. Toothache. Tumors. Vicarious menstruation.
Lobelia Erinus
Menses come on too often, Bearing down. Cancer.
Lobelia Inflata
During menstruation violent pain in sacrum. Violent pain in the sacrum, with fever. Suppression of the menses. Amenorrhea. Dysmenorrhea. Serous discharges from vagina.
Lilium Tigrinum
Bearing down sensation. Sharp or gasping pains in ovarian region. Pains in ovaries extending into inside of thighs. Ovaries sore and painful to touch. Feels pressure on ovaries. Severe neuralgic pain in uterus. Fundus of uterus low down. Leucorrhea, leaving brown spots on clothes.
Medorrhinum
Severe pain in ovaries, sensation of sac in abdomen. Intense, excruciating, neuralgic pains in whole pelvic region, extending downwards through ovarian region to uterus. Profuse menses: dark clotted, stains difficult to wash out; also, bright blood, with faintness and some pain. Intense menstrual colic.
Thuja Occidentalis
Thuja occ is excellent for ovarian cyst, especially left side. Inflammation of left ovary with severe pain , at every menstrual period. The menses is scanty or retarded, too early or too short.
Lycopodium Clavatum
Lycopodium Clavatum is best for right side ovarian cysts. Burning or boring pains may be felt in the ovary. Menses too late; last too long, too profuse. Vagina dry. Coition painful. Right ovarian pain, Ovarian cyst. Varicose veins of pudenda. Leucorrhea, acrid, with burning in vagina. Discharge of blood from genitals during stool. Nymphomania with terrible teasing desire in external organs. Itching, burning, and gnawing in vulva.
Menstruation too late; lasts too long; sometimes suppression of; profuse, protracted; flow partly black, clotted, partly bright red or partly serum; with labor-like pains followed by swooning. Varices on the genitals.
Mercurious
Suppression of catamenia. Catamenia too copious, with uneasiness and colic. Metrorrhagia. Discharge of blood in an old woman, eleven years after menses had ceased. Before catamenia: dry heat, with ebullition of blood, and congestion in head. Congestion of blood to uterus. Inflammation of ovaries and uterus. Purulent, corrosive leucorrhea, with itching in the parts. Hard tubercles on labia majora. Itching pimples, and nodosities in labia. Itching of genitals. Prolapsus uteri. Sterility with too profuse menstruation.
Piper Nigrum 
Ovaries and uterus congested, with pricking and lancinating pains. Contraction of uterus with sensation as if something strove to penetrate into it. Burning and distending pains in uterus. Menses: difficult, retarded; capricious, irregular, with colic and black blood. Cysts. Infections in uterus.
Colocynthis
Boring pain in ovary. Must draw up double, with great restlessness. Round, small cystic tumors in ovaries or broad ligaments. Wants abdomen supported by pressure. Bearing-down cramps, causing her to bend double. Ovarian Cysts.
The pain varies in character, ranging from cramping, stitching to tensive. Burning sensation in the ovaries that gets better upon bending over double and a sensitive ovarian region that seems hard and swollen are the symptoms that indicate the need for this medicine.
Apis Mellifica
Cysts that cause pain during intercourse. A stinging, sharp, cutting pain from the ovary radiating down the thigh, soreness and tenderness over the ovarian region, heaviness in the ovarian region and pain in the ovaries during menstruation. Edema of labia; relieved by cold water. Soreness and stinging pains; ovaritis; worse in right ovary.
Amenorrhea or menorrhagia. Inflammation, induration, swelling, and dropsy of the ovaries. Weight and pain in either ovarian region, predominantly right side. Ovarian cysts. The ovaries feel better by lying on right side. Enlargement of the right ovary with pain in the left pectoral region and cough. Sharp, cutting, stinging pain in the swollen ovary; worse during menstruation.
Ovarian tumors, with stinging pains like bee stings. Metritis, peritonitis, with stinging, thrusting pains. Dropsy of the ovaries; dropsy of the uterus. Threatened miscarriage in the early months. Abortion. Dropsy in the latter part of pregnancy attended with puerperal convulsions. Ulceration and engorgement of os-uteri. Large and painful swelling of the labia, with heat and stinging pains.
Erysipelatous inflammation of the breasts. Swelling and hardness of the mammae threatening to ulcerate. Scirrhous or open cancer of the mammae, with stinging, burning pains. Dysmenorrhea, with severe ovarian pains. Ovarian cysts. Metrorrhagia profuse, with heavy abdomen, faintness, stinging pain. Sense of tightness. Bearing down, as if menses were to appear. Ovarian tumors, metritis with stinging pains. Great tenderness over abdomen and uterine region.
Pulsatilla Nigricans
Nymphomania. Drawing, pressive, spasmodic and contractive pain extending towards uterus with qualmishness, ovarian cysts. Burning (sticking) pain in vagina and pudenda. Metrorrhagia (discharge now stopping, and then stronger again, of coagulated, clotted blood, or with false labour-pains). Menstrual blood black, with clots of mucus, or pale and serous. Catamenia irregular, tardy, or premature, of too short or too long duration, or entirely suppressed, with colic, hysterical spasms in abdomen, hepatic pains, gastralgia, pain in loins, nausea and vomiting, shivering and paleness of face, megrim, vertigo, moral affections, tenesmus of anus and bladder, stitches inside, and many other sufferings before, during, or after period.
Suppression of menses (especially in elderly women in whom they usually occur at full moon). Delay of first menses.
Leucorrhea, thick, like cream. False pregnancy. During pregnancy: nausea, morning sickness; varicose veins, bluish (cyanotic).
Kali Bromatum
Sebaceous cysts. There is ovarian neuralgia with great nervous uneasiness from ungratified sexual desire. Aversion to sex. Pruritus. Ovarian neuralgia with great nervous uneasiness. Exaggerated sexual desire. Cystic tumors of ovaries.
Sabina Officinalis
Almost insatiable desire for coition with corresponding gratification. Sexual desire greatly increased (almost amounting to nymphomania). Contractive pain in region of uterus. Ovarian cysts. Stitches deep in vagina. Sanguineous congestion in uterus. Hemorrhages of partly pale red, partly clotted, or of very thin, discolored, offensive-smelling blood.
Metrorrhagia with discharge of clotted or bright-red blood, and pains resembling labour pains in the sacrum and in the groins. Metrorrhagia, bright blood. Menses continue too long. Menstrual discharge partly fluid, partly clotted and offensive; it may be either bright red or dark and coagulated; flows mostly in paroxysms, which are brought on by slightest motion; or flow ceases when walking about (menses only when lying down).
Suppressed catamenia with very offensive-smelling leucorrhea (like rotten meat). Miscarriage (especially in the third month). Perceptible swelling of mammae. Tingling in mammae. Inflammation of the uterus after parturition. Retained placenta. After-pains with sensitiveness of abdomen.
Sepia Succus
Pelvic organs relaxed. Bearing-down sensation as if everything would escape through vulva, must cross limbs to prevent protrusion, or press against vulva. Leucorrhea yellow, greenish; with much itching. Menses Too late and scanty, irregular; early and profuse; sharp clutching pains. Violent stitches upward in the vagina, from uterus to umbilicus. Ovarian cysts. Prolapse of uterus and vagina. Morning sickness. Vagina painful, especially on coition.
Silica Tera
Menses too early and too feeble, or else too profuse, with paroxysms of icy coldness over whole body. Suppression of the menses. Discharge of blood before proper period; menses too late; protracted; blood acrid. Metrorrhagia. During the menses, pains in the abdomen, pale appearance of objects, or burning sensation and excoriation in vulva. Itching, burning, and soreness in pudenda; during menses. Abortion. Leucorrhea, which flows when urinating, or after the menses. Leucorrhea, like milk, flowing at intervals, and preceded by griping in umbilical region. Acrid, corrosive leucorrhea.
Kreosotum
Premature catamenia, of too long continuance, and too copious, with a discharge of black blood. Appearance of menses during pregnancy. Abdominal spasms; pressure in the genitals; leucorrhoea.
Plumbum Metallicum
Retarded menstruation. Amenorrhea, chloro-anemia. Nymphomania. Wants to stretch limbs during ovarian pains. Spasmodic dysmenorrhea. Cessation of menses on invasion of colic; may reappear after paroxysm, or not again until next period. Metrorrhagia with sensation of strong pulling from abdomen to back; during climacteric, dark clots alternating with fluid blood or bloody serum. Strangulation of prolapsed portion of vagina, intense pain. Mucous discharge per Vagini. Feels a lack of room for fetus in uterus; inability of uterus to expand; threatened abortion.
Prognosis for a woman with ovarian cysts
Most functional (related to the menstrual cycle) ovarian cysts resolve on their own and do not cause long-term problems. Benign cysts or benign tumors can be surgically removed. The vast majority of ovarian cysts do not cause any long-term problems. Rarely, cysts may be present within ovarian cancer. In this case, the prognosis depends upon the extent of spread and the exact type of cancer that is present.
Fresh case of Hemorrhagic Ovarian Cyst 
On 26th June. 2021, lady, age-43, intolerable severe tearing pain in the right-side pelvis, entered in my office in bending position, tenderness in abdomen.
I gave her a dose of Colocynth-1M straight after that she could explain her problem.
From last four months She had painful, offensive, bright red clotted menses, Occasional hot flushes, Weakness, breast pain and irritability before menses, Puffy eyelids, obese.
There was no other gynecological complain.
Sleep disturbed. Pain and stiffness in joints, sometimes difficult to comb her hair as she could not raise her hands (stiffed shoulder), can’t cover feet while sleeping (burning), Likes sweets, Her mother in law was not so cooperative and she had to suppress anger and emotions.
I advised US abdomen/Pelvis.
Ultrasound reports showed a hemorrhagic cyst of 4.3 by 2.4 cm in the right ovary.
Diagnosis :
Her mental picture especially suppressed anger indicated Staphysagria.
Obese woman, menopausal age, stiff joints and muscles, infiltration in face, painful menses accompanied by ovarian complaints, hemorrhagic cyst in right ovary, warm blooded patient was indicating Apis mel.
But We have to cover the chief complaint that is SEVERE PAIN…… Kali Iodatum ?
My Prescription Dr Qaisar Ahmed for Twenty days was:
- Kali iodatum-200 TDs
- Apis Melifistida-200 TDs
- Silicea-200 TDs
- Arsenicum Album-200 TDs
- Colocynth-200 TDs
She said- “After your medicine, skin eruption with severe itching came on my spine.
Refer for repeat US abdomen/pelvis on 16th july 2021; In US no abnormalities were found. She was absolutely normal.
I was amazed too because Hemorrhagic ovarian cysts usually dissolve within 8-10 weeks in premenopausal woman.
P. S: This article is only for doctors having good knowledge about Homeopathy and allopathy, for learning purpose(s).
For proper consultation and treatment, please visit our clinic.
None of above-mentioned medicine(s) is/are the full/complete treatment, but just hints for treatment; every patient has his/her own constitutional medicine.
To order medicine by courier, please send your details at WhatsApp– +923119884588
 Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Senior research officer at Dnepropetrovsk state medical academy Ukraine.
Location: Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Find more about Dr Sayed Qaisar Ahmed at:
https://www.youtube.com/Dr Qaisar Ahmed
Great goods from you, man. I have understand your stuff previous to and you’re just extremely magnificent. I actually like what you’ve acquired here, really like what you are stating and the way in which you say it. You make it entertaining and you still care for to keep it sensible. I can’t wait to read much more from you. This is actually a terrific site.
I was just searching for this info for a while. After 6 hours of continuous Googleing, at last I got it in your web site. I wonder what is the lack of Google strategy that don’t rank this type of informative sites in top of the list. Generally the top sites are full of garbage.
Wow! This blog looks just like my old one! It’s on a completely different topic but it has pretty much the same layout and design. Great choice of colors!